
Atrial Fibrillation
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia — affecting over 33 million people worldwide. Characterized by an irregular, chaotic electrical rhythm in the upper heart chambers, its principal danger is cardioembolic stroke.
What Is Atrial Fibrillation?
Atrial fibrillation (AF) replaces normal, coordinated contraction of the upper heart chambers with rapid, chaotic quivering.
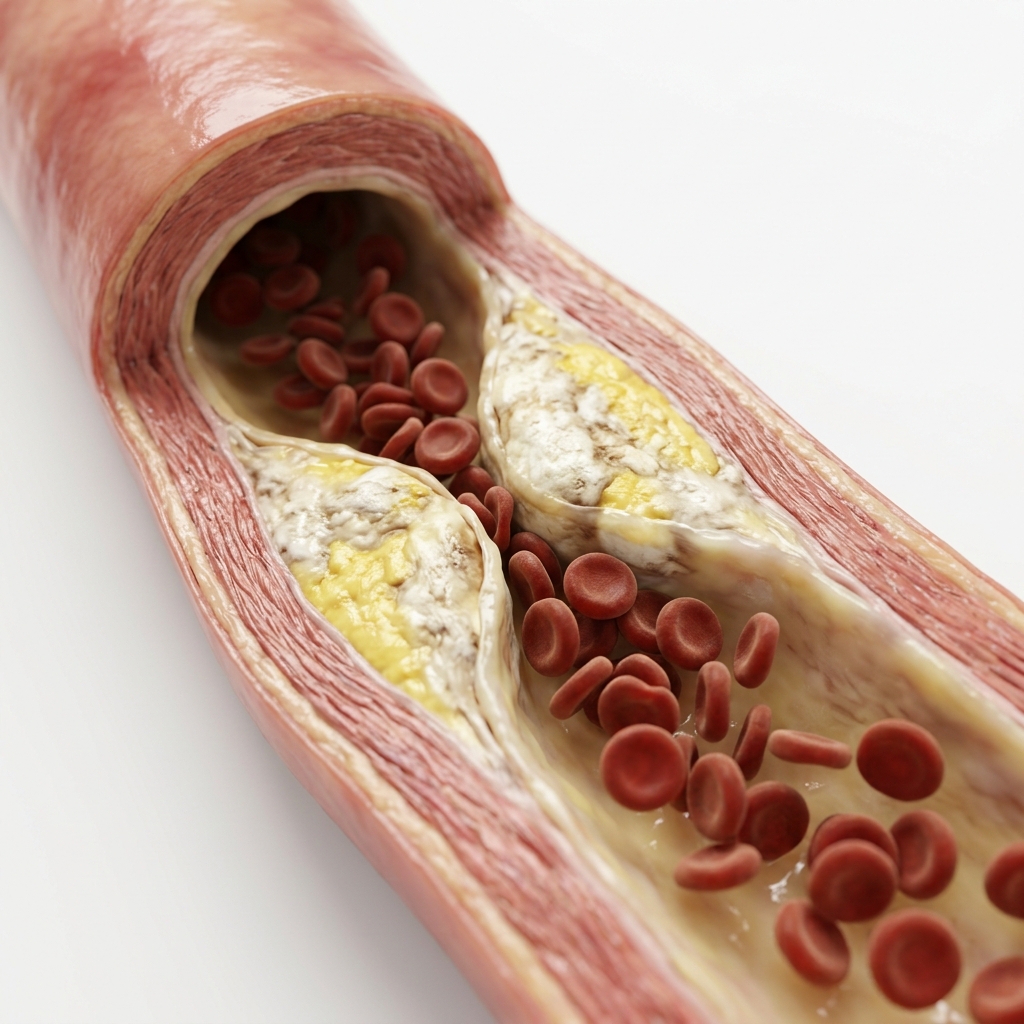
Instead of beating in rhythm, the upper chambers quiver, preventing blood from moving fully into the ventricles. Stagnant blood in the left atrial appendage easily clots, creating a massive risk of thromboembolic stroke.
Causes & Risk Factors for Atrial Fibrillation
Multiple cardiovascular and systemic conditions predispose to atrial fibrillation.
Hypertension
The strongest risk factor for AF. Hypertensive LVH and left atrial dilation create the electrophysiological substrate. Chronic pressure overload leads to atrial fibrosis.
Heart Failure
Elevated filling pressures and atrial stretch promote AF. AF and heart failure form a vicious cycle — each worsening the other.
Older Age
AF prevalence increases with age. Age ≥75 years carries double weight in CHA₂DS₂-VASc scoring due to exponentially rising stroke risk.
Valvular Heart Disease
Mitral stenosis and regurgitation cause left atrial enlargement. Rheumatic mitral stenosis in India is a particularly common cause of AF.
Obesity & Sleep Apnoea
Obesity causes atrial dilatation and inflammation. Obstructive sleep apnoea triggers nocturnal hypoxaemia and sympathetic surges that provoke AF episodes.
Diabetes & Thyroid Disease
Diabetes increases AF risk by ~40%. Hyperthyroidism directly causes AF through increased sympathetic tone and atrial automaticity.
Classification of Atrial Fibrillation
We categorize AF by episode duration and pattern to guide optimal rate or rhythm interventions.
Classic Symptoms & Presentations
AF presents on a wide spectrum, from silent, asymptomatic quivering to acute cardioembolic strokes.
Palpitations
Racing, fluttering, or irregular heartbeat sensation. May be persistent or episodic. Many patients describe a 'flip-flop' or irregularly irregular thumping. Some patients feel nothing at all — AF is silent in approximately 30% of cases.
Breathlessness or Reduced Exercise Tolerance
Loss of atrial contraction reduces cardiac output by 15–25%, causing effort intolerance, dyspnoea on exertion, or fatigue that patients often attribute to age or fitness.
Dizziness or Presyncope
Especially during rapid AF (ventricular rate >130 bpm). Rarely causes blackout without concurrent structural heart disease.
Stroke as First Presentation
In 15–20% of AF patients, the condition is first detected when they present with acute stroke or TIA. CRYSTAL AF trial showed ILR detects AF in 30% of cryptogenic stroke patients at 3 years.
How Is Atrial Fibrillation Diagnosed?
Standard cardiac screening to record electrical events and identify structural causes.
Resting 12-Lead ECG
First test. Captures AF as an irregularly irregular baseline with absent P waves and fibrillatory waves. If symptoms are present during recording, the diagnosis is confirmed.
24-Hour Holter Monitoring
Continuous ECG for 24–48 hours captures paroxysmal AF that resting ECG misses. Symptom diary correlation confirms whether palpitations coincide with AF.
2D Echocardiography
Assesses left atrial size, ejection fraction, valve disease, and structural cause of AF. Essential first workup before deciding on anticoagulation and rhythm control.
CHA₂DS₂-VASc Stroke Risk Scoring
Validated clinical scoring framework used to calculate annual stroke probability and determine if oral anticoagulation is indicated.
Extended Monitoring (if needed)
If standard Holter is normal but episodes are infrequent, 7-day patch monitoring or implantable loop recorder (ILR) detects paroxysmal AF. CRYSTAL AF showed ILR detects AF in 30% at 3 years.
What Happens If Left Untreated?
Untreated AF significantly increases the risk of stroke, heart failure, and cognitive decline.
Cardioembolic Stroke
Stagnant blood in the left atrial appendage forms clots that can embolise to the brain. AF causes 20–30% of all ischaemic strokes. Risk is 5× higher than without AF.
Tachycardia-Mediated Cardiomyopathy
Chronic rapid ventricular rates (>110 bpm) can cause LV dysfunction and heart failure — reversible with rate or rhythm control.
Heart Failure Worsening
Loss of atrial contraction reduces cardiac output. AF in patients with existing HF accelerates decompensation and hospitalisation.
Cognitive Decline & Dementia
AF is associated with increased risk of cognitive impairment and vascular dementia, independent of clinical stroke, due to silent cerebral microemboli.
The Three Pillars of Atrial Fibrillation Management
Optimal clinical strategies address simultaneous pathways to guarantee stroke prevention and symptom control.
Stroke Prevention — Anticoagulation
ARISTOTLE: Apixaban −21% stroke, −31% major bleeding vs warfarinAll patients with CHA₂DS₂-VASc ≥2 (men) / ≥3 (women). DOACs are preferred for non-valvular AF — at least as effective as warfarin, lower ICH risk, no INR monitoring. Aspirin is NOT an alternative.
Rate Control
RACE 2 (NEJM 2010): HR <110 bpm non-inferiorSlows ventricular response using beta-blockers, CCBs, or digoxin. Lenient target (resting HR <110 bpm) is non-inferior to strict control (RACE 2).
Rhythm Control
EAST-AFNET 4: −21% CV events · CASTLE-AF: −38% death/HF in HFrEFRestores sinus rhythm via cardioversion, antiarrhythmic drugs, or catheter ablation. EAST-AFNET 4 showed early rhythm control reduced CV events by 21%.
DOAC Blood Thinner Comparison
Direct Oral Anticoagulants (DOACs) are standard-of-care for non-valvular AF, offering massive reductions in stroke with low bleeding rates.
Lifestyle Changes & Self-Care for AF
Lifestyle modifications can reduce AF burden and improve symptom control.
Avoid Alcohol Triggers
Reduces episode frequencyAlcohol is a well-established trigger for AF episodes. The 'Holiday Heart Syndrome' describes AF after binge drinking. Limit to 1–2 units per day or abstain entirely.
Optimize Sleep & Manage Sleep Apnoea
CPAP: −42% AF recurrenceObstructive sleep apnoea is a strong independent risk factor for AF. CPAP therapy reduces AF recurrence after cardioversion and ablation.
Weight Management
10% weight loss: −6× AF-free survivalObesity causes atrial dilatation and inflammation. Weight loss of 10% or more significantly reduces AF burden and progression from paroxysmal to persistent.
Stress Reduction & Vagal Tone
Complementary therapyStress and anxiety can provoke AF episodes. Yoga, meditation, and biofeedback have been shown to reduce episode frequency.
Regular Moderate Exercise
Improves quality of lifeRegular aerobic exercise maintains cardiovascular fitness and helps maintain sinus rhythm. Avoid extreme endurance exercise which may increase AF risk.
Monitor Triggers
Personalised trigger avoidanceKeep a symptom diary to identify personal triggers — caffeine, alcohol, stress, dehydration, or certain medications. Avoid identified triggers.
Guidelines & Latest Evidence
Major trials define the modern management of atrial fibrillation.
When to See a Doctor
Certain AF symptoms and presentations require prompt medical evaluation.
New-Onset Palpitations or Irregular Pulse
Any new sensation of irregular, rapid, or 'fluttering' heartbeat warrants ECG and evaluation for AF.
Symptoms of Stroke or TIA
Sudden weakness, facial droop, speech difficulty, or visual loss may be the first presentation of AF. Immediate emergency assessment is required.
Rapid Heart Rate at Rest
If the resting heart rate is consistently >120 bpm or you feel dizzy/lightheaded, seek evaluation for rate control.
Bleeding While on Anticoagulation
Any unusual bleeding, easy bruising, dark stools, or blood in urine while on DOACs or warfarin requires assessment of anticoagulation intensity.
Frequently Asked Questions
Guideline-directed clarifications regarding chronic irregular rhythms and stroke safety.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia — an irregular, chaotic electrical rhythm in the upper heart chambers (atria). Instead of contracting in an organised way, the atria quiver, causing an irregularly irregular pulse. The principal danger is stroke: stagnant blood in the left atrial appendage forms clots that can embolise to the brain. AF causes 20–30% of all ischaemic strokes. Every patient with AF requires CHA₂DS₂-VASc stroke risk scoring and anticoagulation where indicated.
The CHA₂DS₂-VASc score calculates annual stroke risk in non-valvular AF patients. Risk factors and their points: Heart failure (1), Hypertension (1), Age ≥75 (2 — double weight), Diabetes (1), Stroke/TIA history (2 — double weight), Vascular disease (1), Age 65–74 (1), Female sex (1). Maximum score = 9. Men with score ≥2 and women with score ≥3 should receive anticoagulation. Prior stroke or TIA (S₂ = 2 points) alone mandates anticoagulation regardless of other factors.
Rate control slows the ventricular rate (target <110 bpm at rest) using beta-blockers or diltiazem — the patient remains in AF but symptoms are controlled. Rhythm control attempts to restore and maintain normal sinus rhythm via cardioversion, antiarrhythmic drugs, or catheter ablation. EAST-AFNET 4 (NEJM 2020) showed that early rhythm control in patients with cardiovascular risk factors reduced CV death, stroke, and hospitalisation by 21% versus rate control alone — supporting earlier rhythm control in suitable patients.
DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) are the preferred anticoagulants for non-valvular AF — safer and more effective than warfarin for most patients. They are at least as effective at stroke prevention, with significantly lower intracranial haemorrhage risk. ARISTOTLE showed apixaban reduced stroke by 21%, all-cause mortality by 11%, and major bleeding by 31% versus warfarin. DOACs do not require INR monitoring. Warfarin remains indicated for mechanical heart valves and significant mitral stenosis.
Yes — paroxysmal AF is defined as episodes that start and stop spontaneously within 7 days, often lasting minutes to hours. Many patients with paroxysmal AF experience symptoms intermittently, sometimes going weeks or months between episodes. These brief episodes carry the same stroke risk as persistent AF if CHA₂DS₂-VASc score is elevated, so anticoagulation decisions are based on risk factors, not on whether the AF is constant or intermittent. Holter monitoring is essential to capture paroxysmal episodes — a single normal ECG does not rule out AF. Approximately 30% of patients with paroxysmal AF will progress to persistent or permanent AF within 5 years.
Common triggers for AF episodes include excessive alcohol consumption (particularly binge drinking — the 'holiday heart syndrome'), caffeine in sensitive individuals, sleep deprivation, physical or emotional stress, dehydration, and electrolyte imbalances. Fever, acute infections (especially pneumonia), and post-surgical states can also precipitate AF. Obstructive sleep apnoea is a powerful and under-recognised trigger — treating sleep apnoea can significantly reduce AF burden. Some patients identify specific triggers through symptom diaries. Avoiding known triggers, maintaining good sleep hygiene, and managing stress can reduce episode frequency but does not eliminate the need for anticoagulation if indicated.
Catheter ablation (pulmonary vein isolation) is more effective than antiarrhythmic medication at maintaining sinus rhythm and reducing AF recurrence — particularly in patients with paroxysmal AF and structurally normal hearts. The EAST-AFNET 4 trial showed that early rhythm control (including ablation) reduced cardiovascular death, stroke, and hospitalisation by 21% compared with rate control alone. Ablation is especially beneficial for patients who are intolerant of or unresponsive to antiarrhythmic drugs, those with heart failure and AF (CASTLE-AF showed a 38% reduction in death and HF hospitalisation), and younger patients who prefer a curative approach. However, ablation does not eliminate the need for anticoagulation in patients with elevated stroke risk.
Yes — with appropriate management, most patients with AF can lead a full, active, and normal life. The key components are: stroke prevention with anticoagulation when indicated (DOACs are safe and convenient with no need for regular blood monitoring), rate or rhythm control to manage symptoms, and treatment of underlying conditions such as hypertension, sleep apnoea, and obesity. Many athletes, public figures, and active seniors live well with AF. Regular exercise is encouraged, though competitive athletes should undergo cardiac evaluation. Driving is generally permitted if symptoms are controlled. The most important message is that AF is a manageable chronic condition — not a life sentence.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.
24-Hour Holter Monitor
Continuous ECG recording capturing paroxysmal AF and quantifying AF burden.

2D Echocardiography
LA size assessment, LV function, and structural cause evaluation for AF.

Pacemaker Implantation
CRT and pacemaker solutions for AF with sick sinus or AV block.
Coronary Artery Disease
CAD frequently coexists with AF — comprehensive joint management.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.