Coronary Artery Disease
Coronary artery disease (CAD) — commonly called 'heart blockage' — is the progressive narrowing of the coronary arteries by atherosclerotic plaque. It is the leading cause of death in India and the most common reason patients need coronary angiography, angioplasty, and bypass surgery.
The Pathology of Heart Blockage
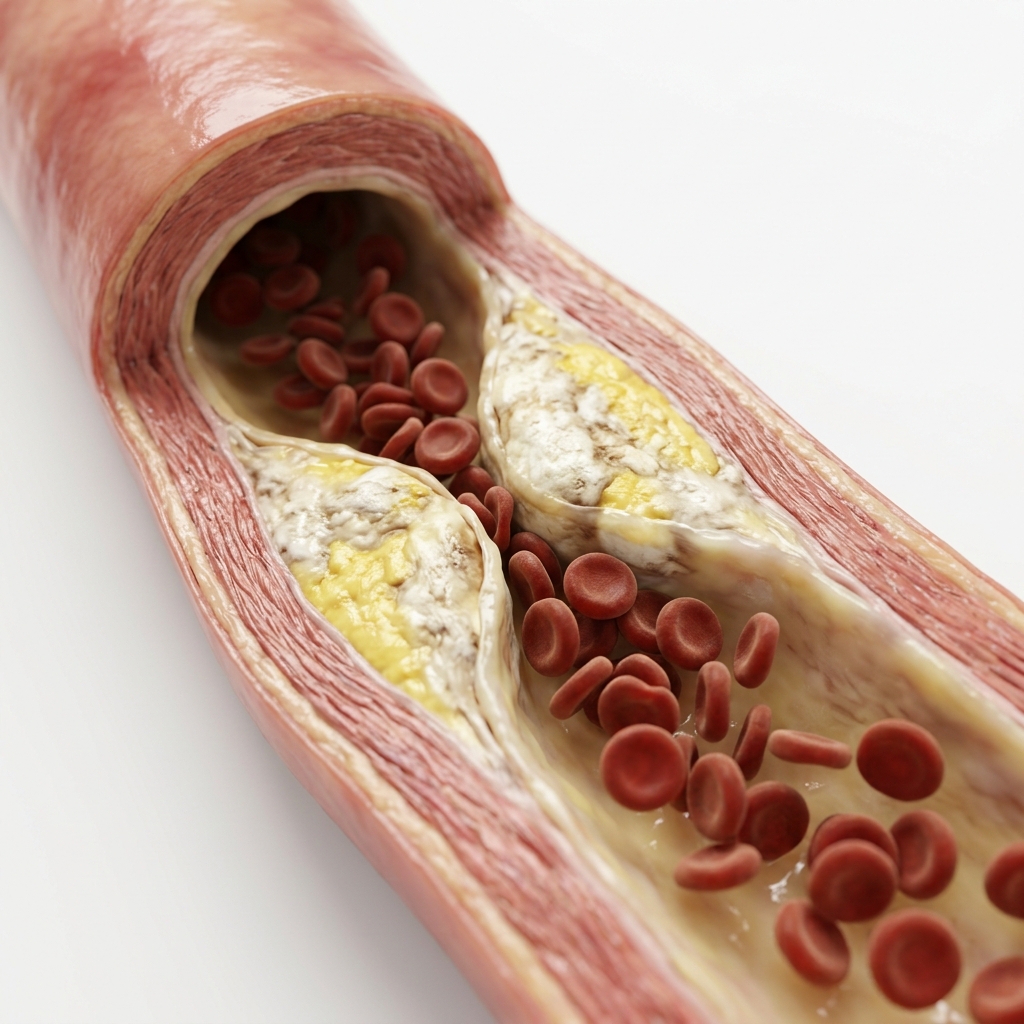
Coronary artery disease occurs due to the progressive accumulation of cholesterol plaques inside the arteries feeding your heart.
Over decades, inflammatory responses and lipids turn into calcified plaques that harden and narrow the artery lumen. This severely limits the blood supply, manifesting as exercise-induced tightness (stable angina) or leading to absolute emergency blockages (heart attack) if a plaque ruptures and a thrombus forms.
Causes & Risk Factors for Coronary Artery Disease
CAD results from a combination of modifiable and non-modifiable risk factors.
Hypertension
Chronically elevated BP accelerates endothelial injury and plaque formation. Systolic >130 mmHg doubles CAD risk.
Dyslipidaemia
Elevated LDL is the primary driver of plaque formation. Each 1 mmol/L reduction in LDL reduces major CV events by ~20%.
Diabetes Mellitus
Doubles CAD risk. Causes diffuse, small-vessel disease — often multi-vessel, favouring CABG over PCI in complex cases.
Smoking
Most powerful single preventable risk factor. 2–4× increased CAD risk. Risk halves within 1 year of cessation.
Age & Family History
Risk increases with age. Men develop CAD 7–10 years earlier than women. First-degree relative with early CAD doubles personal risk.
Obesity & Physical Inactivity
Obesity drives hypertension, diabetes, and dyslipidaemia. Physical inactivity independently increases CAD risk by 50–100%.
The Coronary Artery Disease Spectrum
CAD exists on a dynamic clinical spectrum from chronic, manageable symptoms to acute, life-threatening events.
Symptoms & Risk Stratification
Identifying the clinical warnings early can prevent irreversible heart muscle damage or sudden cardiac arrest.
Chest Pain, Pressure, or Tightness
The hallmark symptom. Central or left-sided, radiating to arm, jaw, or back. Provoked by exertion, relieved by rest (stable) or persists (ACS).
Breathlessness on Exertion
May be the predominant symptom — especially in diabetics, elderly, and women who may have 'silent' CAD without classic chest pain.
Profuse Sweating (Diaphoresis)
Cold, clammy sweating during chest symptoms is a warning sign of significant cardiac event. Do not attribute to heat or anxiety.
Nausea, Dizziness, or Jaw/Arm Pain
Inferior MI commonly presents with epigastric pain, nausea, and vomiting — frequently misdiagnosed as acid reflux.
Palpitations or Sudden Loss of Consciousness
Acute ischaemia can trigger VT or VF. Palpitations or syncope with chest pain requires immediate emergency assessment.
How Is Coronary Artery Disease Diagnosed?
We employ a structured cascade of tests from non-invasive screening to definitive angiography.
Resting 12-Lead ECG
First test. Detects ST changes (ischaemia), Q waves (prior MI), LVH, and arrhythmias. A normal resting ECG does not rule out CAD.
High-Sensitivity Troponin
Cardiac biomarkers that rise within 1–3 hours of myocardial injury. Essential for diagnosing NSTEMI and guiding urgent angiography.
2D Echocardiography
Detects regional wall motion abnormalities, LV function, and structural complications of MI. Stress echo can induce and visualise ischaemia.
CT Coronary Angiography (CTCA)
Non-invasive imaging of coronary anatomy. High negative predictive value — a normal CTCA effectively rules out obstructive CAD.
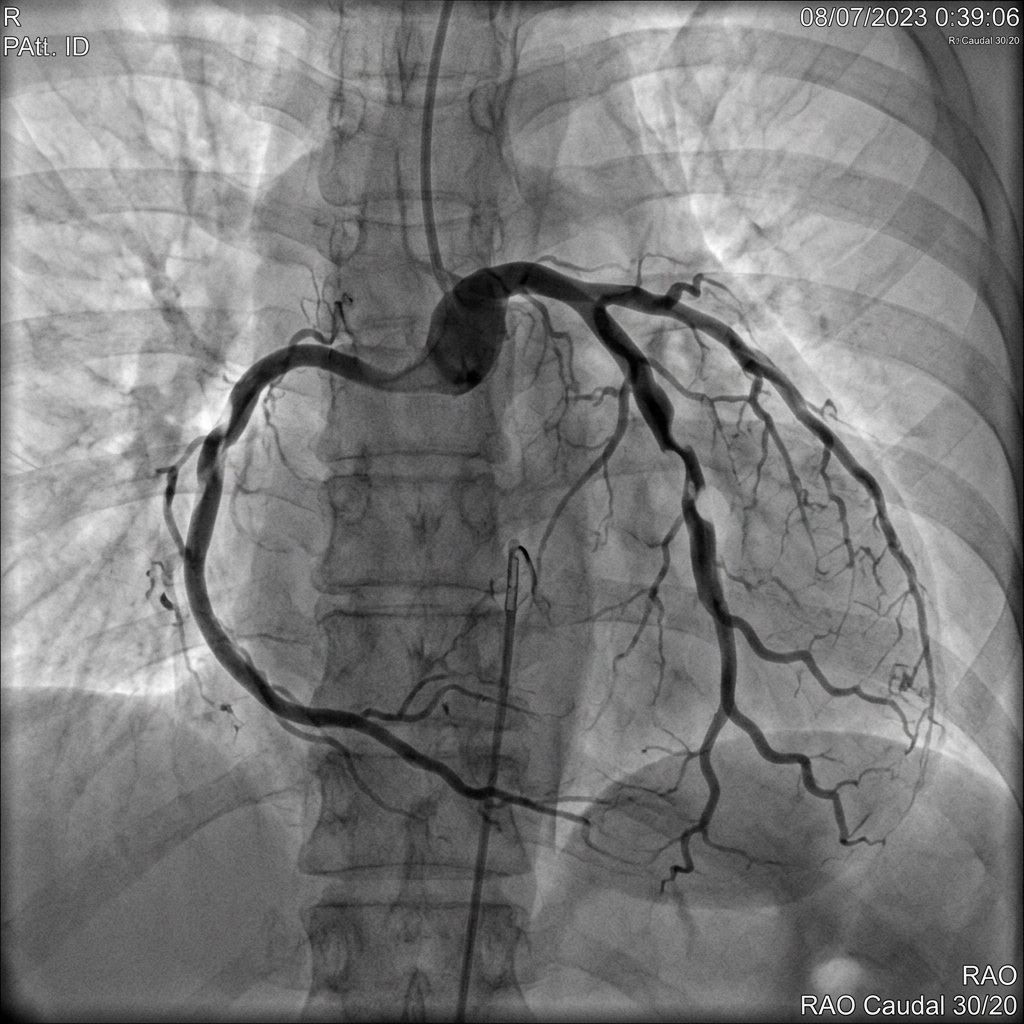
Invasive Coronary Angiography with FFR/IVUS
Gold standard. Catheter-based dye injection visualises stenosis. FFR measures physiological significance. IVUS/OCT guides optimal stent placement.
What Happens If Left Untreated?
Progressive CAD leads to worsening symptoms, heart attack, heart failure, and death.
Myocardial Infarction (Heart Attack)
Plaque rupture with thrombus formation causes complete coronary occlusion. Without timely PCI, irreversible myocardial necrosis occurs.
Heart Failure
Extensive or repeated MI reduces LV function, leading to symptomatic HF, reduced exercise capacity, and poor prognosis.
Stroke
CAD is a marker of systemic atherosclerosis. Many patients with CAD also have carotid disease increasing stroke risk.
Sudden Cardiac Death
Acute ischaemia can trigger lethal ventricular arrhythmias. VF is the first presentation of CAD in many patients.
Evidence-Based Treatment Pathways
Therapy is tailored according to international guidelines and anatomically calculated scores.
Guideline-Directed Medical Therapy
ESC 2019 · AHA/ACC 2021Antiplatelet (aspirin ± clopidogrel), high-intensity statin (LDL <1.4 mmol/L), beta-blocker, ACEi/ARB, nitrates. The foundation for all CAD patients.
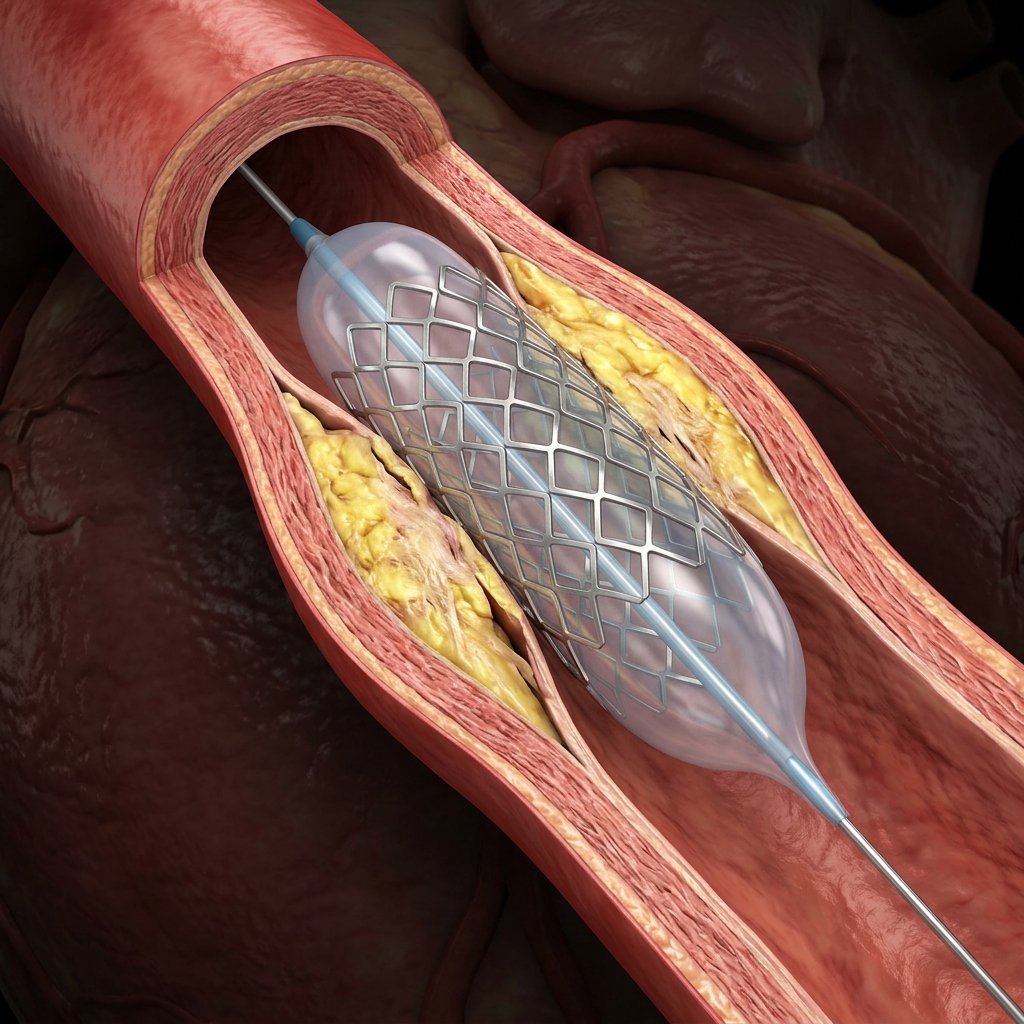
Coronary Angioplasty & Stenting (PCI)
RIVAL: −73% bleeding · FAME 2: FFR-guided PCIBalloon angioplasty + drug-eluting stent via radial artery. IVUS/OCT guidance reduces MACE by 25% (RENOVATE). FFR-guided to ensure haemodynamic significance.
Coronary Artery Bypass Surgery (CABG)
SYNTAX: CABG superior for complex 3VDFor complex three-vessel disease, left main disease, and diabetics with multi-vessel CAD. SYNTAX score guides decision. Heart Team approach.
Guideline-Directed Medical Therapy for CAD
Medical therapy is the cornerstone of CAD management for all patients.
Lifestyle Changes & Risk Factor Modification
Lifestyle interventions are the cornerstone of secondary prevention for coronary disease.
Smoking Cessation
−50% CV risk within 1 yearThe single most effective preventive measure. Risk of MI declines by 50% within 1 year of quitting. Nicotine replacement and counselling improve success.
Heart-Healthy Diet
Reduces MACE by 25–30%Mediterranean diet rich in fruits, vegetables, whole grains, olive oil, and fish. Low in saturated fat, red meat, and processed foods.
Regular Exercise
150 min/week moderate exerciseAt least 150 minutes/week of moderate aerobic activity. Cardiac rehabilitation programs improve outcomes after ACS.
Weight Optimisation
BMI target <25 kg/m²Target BMI 18.5–25 kg/m². Weight loss improves BP, lipids, glycaemic control, and reduces angina symptoms.
Limit Alcohol
Maximum 14 units/weekAlcohol raises BP and provides no cardiovascular benefit. Limit to 1–2 units per day maximum.
Blood Pressure & Diabetes Control
BP <130/80 · HbA1c <7.0%Target BP <130/80 mmHg. HbA1c <7.0% in diabetics. Regular medication adherence is essential for event prevention.
Deciding Between PCI and CABG
We leverage the international SYNTAX score criteria to guide the medical recommendation objectively.
When to See a Doctor
Certain symptoms require immediate medical evaluation to prevent heart attack.
New or Worsening Chest Pain
Any new chest tightness, pressure, or pain, especially if it occurs with less exertion or at rest, requires urgent evaluation.
Chest Pain with Sweating or Nausea
Diaphoresis and nausea during chest pain indicate significant myocardial ischaemia — call emergency services immediately.
Shortness of Breath in a Diabetic
Breathlessness without chest pain may be the only sign of ACS in diabetes. Do not ignore — seek urgent cardiac assessment.
Palpitations or Dizziness with Chest Symptoms
Palpitations, near-fainting, or fainting with chest pain may indicate VT or haemodynamic compromise requiring emergency care.
Frequently Asked Questions
Clinical clarifications regarding heart blockages and management.
Coronary artery disease (CAD) is the progressive narrowing of the arteries supplying the heart muscle by atherosclerotic plaque — a build-up of cholesterol, inflammatory cells, and calcium inside the artery wall. This narrowing reduces blood flow to the heart, causing exertional chest pain (stable angina) or, when a plaque ruptures and triggers a clot, a heart attack. CAD is the leading cause of death in India and worldwide, and is the most common reason for coronary angiography, angioplasty, and bypass surgery.
Stable angina is predictable chest tightness on exertion that relieves at rest — caused by a fixed narrowing. Unstable angina is new or worsening rest pain from a partially ruptured plaque — a cardiological emergency. NSTEMI is a heart attack with elevated troponin but no ST elevation on ECG — partial artery blockage with muscle damage. STEMI is a complete coronary artery occlusion causing ST elevation on ECG — the most severe type requiring emergency angioplasty within 90–120 minutes.
Coronary angioplasty (PCI) is a catheter-based procedure that opens narrowed coronary arteries using a balloon and implants a drug-eluting stent to keep the artery open. No open-chest surgery is required. It is the treatment of choice for STEMI (emergency PCI within 90 minutes), high-risk ACS, and stable angina with ischaemia that is not controlled by medications. At Heartwise Cardiology, all PCI is performed via the radial artery (wrist access) with IVUS or OCT imaging guidance and FFR measurement — providing the highest quality of stent implantation and ensuring stenting is restricted to physiologically significant lesions.
Angioplasty (PCI) opens the blocked artery from inside via catheter — no chest opening, 24–48 hour discharge. Bypass surgery (CABG) creates new vessels that bypass the blocked segments — requires open-chest surgery and 5–7 day stay. CABG is preferred for complex three-vessel disease (SYNTAX score >32), left main disease with high complexity, and diabetics with multi-vessel CAD. PCI is preferred for single-vessel disease, selected two-vessel disease, and low-complexity left main disease. The decision is made jointly by the cardiologist and cardiac surgeon based on the SYNTAX score and clinical factors.
Coronary stents have evolved significantly over the past two decades. Bare-metal stents (BMS) were the first generation — effective at holding arteries open but had high rates of restenosis (re-narrowing) of 20–30%. Drug-eluting stents (DES) are coated with medications that prevent scar tissue from growing through the stent, reducing restenosis to under 5%. Modern DES use biodegradable polymers or polymer-free coatings that reduce the risk of very late stent thrombosis. Bioresorbable scaffolds were designed to dissolve completely over 2–3 years but had higher complication rates and are now rarely used. At Heartwise Cardiology, all stenting is performed with contemporary drug-eluting stents guided by IVUS or OCT imaging to ensure optimal expansion and apposition.
Coronary artery disease can be stabilised and, in some cases, modest plaque regression can be achieved with aggressive risk factor management. High-intensity statin therapy can reduce LDL cholesterol to very low levels, which halts plaque progression and can cause mild plaque regression (reduction in plaque volume by 5–10% over 1–2 years). Lifestyle changes — including smoking cessation, the Mediterranean diet, regular exercise, and weight loss — further stabilise plaques by reducing inflammation and improving endothelial function. However, advanced calcified plaques and established blockages do not fully disappear. The goal of treatment is plaque stabilisation (making plaques less likely to rupture and cause heart attacks) combined with revascularisation (stenting or bypass) for flow-limiting blockages.
After a drug-eluting stent is placed, dual antiplatelet therapy (DAPT — typically aspirin plus a P2Y12 inhibitor such as clopidogrel, ticagrelor, or prasugrel) is required to prevent stent thrombosis — a rare but catastrophic complication where a clot forms inside the stent. For patients with stable CAD, DAPT is recommended for at least 6 months, after which aspirin alone is continued lifelong. For patients who had a heart attack (NSTEMI or STEMI), DAPT is needed for at least 12 months. Patients at high bleeding risk (elderly, kidney disease, history of bleeding) may require shorter DAPT durations. After 12 months, most patients continue single antiplatelet therapy (aspirin or clopidogrel) lifelong.
CT coronary angiography (CTCA) is a non-invasive scan that uses a CT scanner with contrast dye to visualise the coronary arteries. It takes about 15 minutes, can be done as an outpatient, and requires only an IV line in the arm. CTCA is excellent for ruling out coronary artery disease — a normal scan has a negative predictive value of over 95%. It can identify plaque and estimate stenosis severity but cannot treat blockages. Traditional invasive coronary angiography is a catheter procedure where a thin tube is inserted via the wrist (radial artery) and contrast is injected directly into the coronary arteries. It is slightly more accurate for severe stenoses, allows FFR measurement to assess physiological significance of blockages, and can be immediately followed by angioplasty and stenting if needed. CTCA is typically used first for low-to-intermediate risk patients; invasive angiography is reserved for high-risk patients or those with positive non-invasive tests.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.
Coronary Angiography
Diagnostic gold standard — identifies blockages with FFR and IVUS guidance.
Coronary Angioplasty
Radial-access PCI with drug-eluting stents and IVUS/OCT imaging.

Treadmill Stress Test
Exercise ECG to detect ischaemia with Duke Treadmill Score.

Heart Failure
Post-MI heart failure management and ischaemic cardiomyopathy care.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.