Coronary Angiography in Navi Mumbai
Everything you need to know — the procedure, preparation, what results mean, and when you need it — explained by your Interventional Cardiologist.
What Is Coronary Angiography?
A detailed explanation of the gold-standard diagnostic test for coronary artery disease — how it works, what it shows, and why it is the definitive test for coronary blockages.
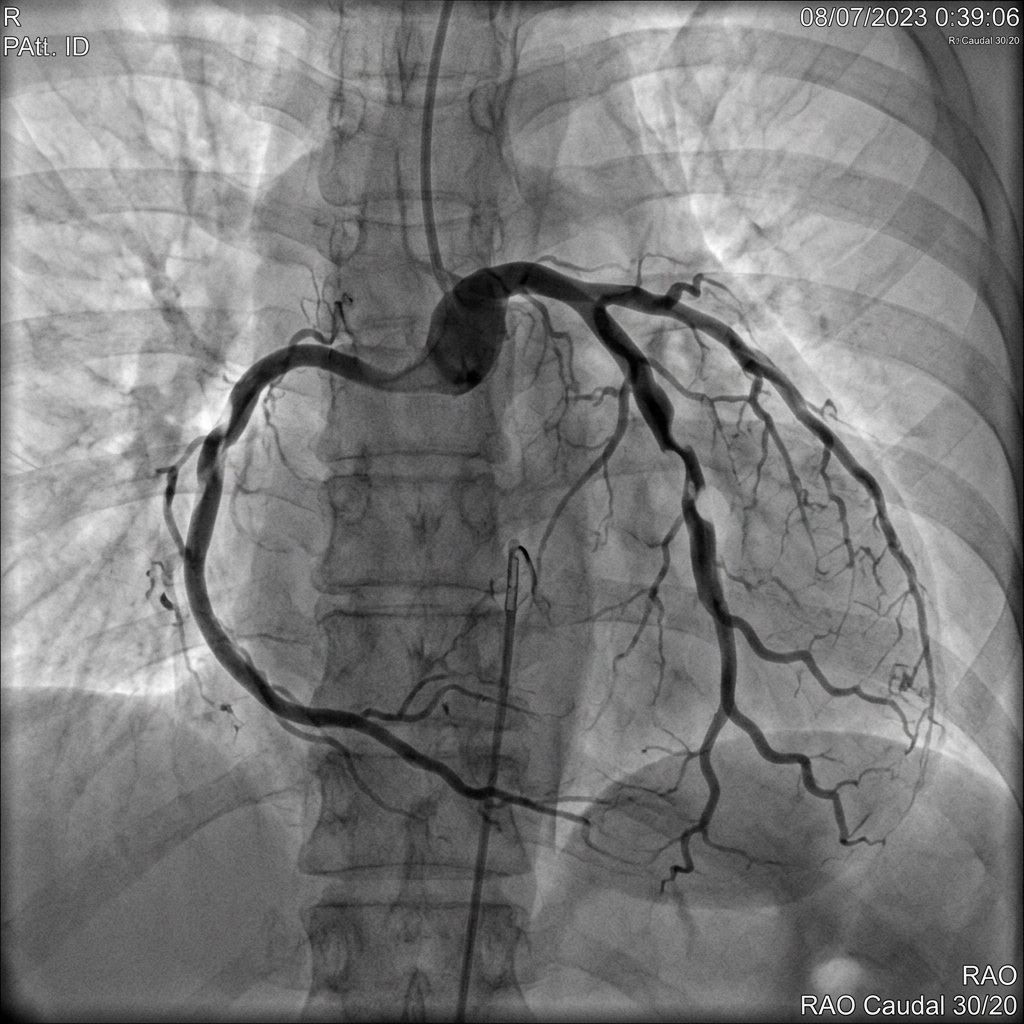
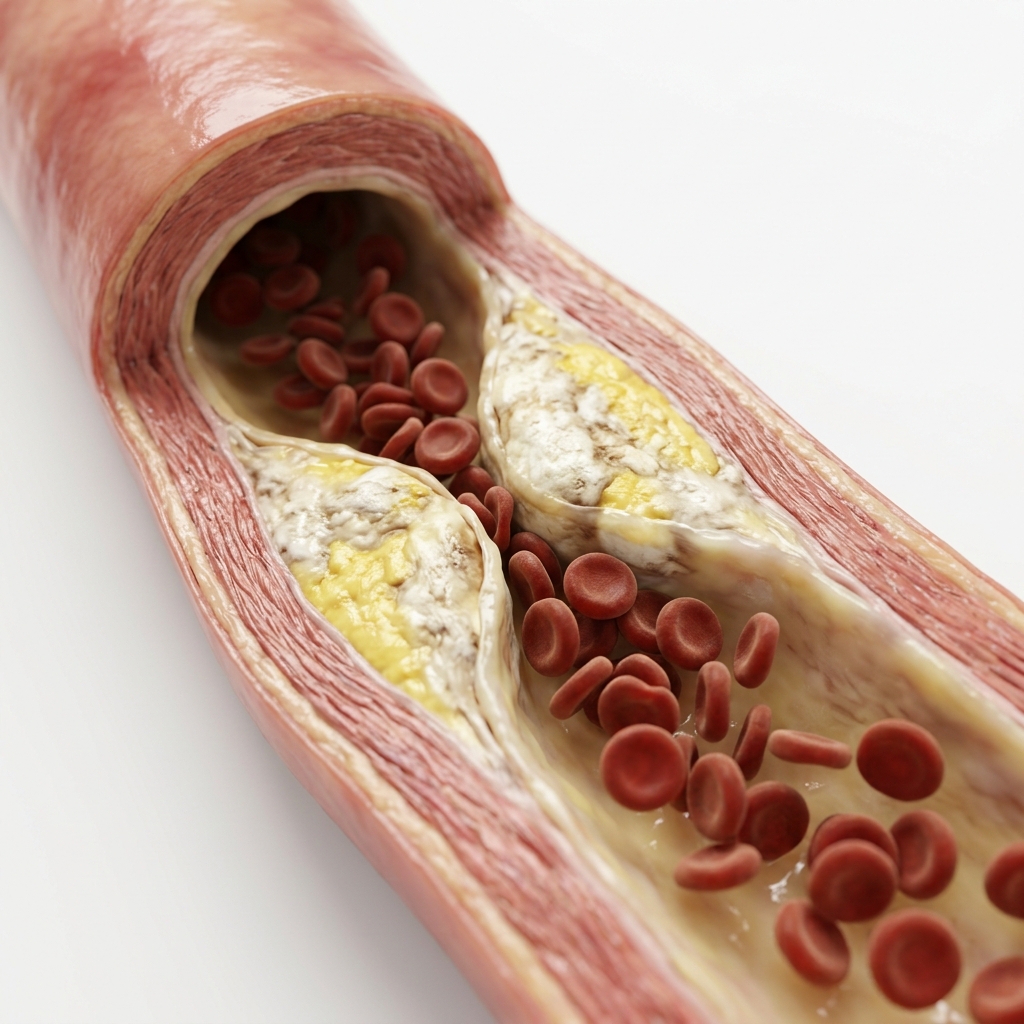
Coronary angiography — also called cardiac catheterisation or coronary arteriography — is a diagnostic imaging procedure that allows the cardiologist to examine the coronary arteries directly. It works by injecting a radiopaque contrast dye into the coronary circulation and capturing real-time X-ray images (called fluoroscopy) as the dye flows through each artery. Any narrowing, blockage, or abnormality in the vessel becomes immediately visible. The coronary arteries are three main vessels — the left anterior descending (LAD), the left circumflex (LCX), and the right coronary artery (RCA) — that deliver oxygenated blood to the entire heart muscle. When any of these arteries become narrowed due to atherosclerotic plaque buildup, the heart muscle downstream is deprived of oxygen, producing symptoms ranging from exertional chest pain (angina) to a heart attack.
Diagnostic accuracy of coronary angiography for significant CAD
ACC/AHA GuidelinesTypical procedure duration for diagnostic angiography
Standard clinical practiceMajor complication rate at experienced interventional centres
ESC Guidelines 2023Why Is Coronary Angiography Needed?
The clinical scenarios in which coronary angiography is indicated — from emergencies to elective assessments.
A cardiologist will recommend coronary angiography when there is a high suspicion of significant coronary artery disease, or when non-invasive tests have returned inconclusive or abnormal results. The procedure provides information that cannot be obtained in any other way: the precise anatomy of each coronary artery, the exact location and degree of narrowing, and whether the blockage is amenable to treatment by angioplasty or requires bypass surgery.
The Radial Approach: Why It Matters
Radial (wrist) versus femoral (groin) access — the evidence behind the preference at Heartwise Cardiology.
How to Prepare for Coronary Angiography
Proper preparation is essential for a safe procedure. Follow these steps before your angiography.
What Happens During Coronary Angiography?
A step-by-step walkthrough of the angiography procedure — from arrival in the Cath Lab to recovery.
Arrival and Preparation (30–45 min before)
An intravenous (IV) cannula is placed in your arm. You are connected to continuous ECG monitoring and pulse oximetry. Local anaesthetic cream is applied to the wrist. The access site is cleaned and draped in a sterile manner.
Local Anaesthesia and Arterial Access
Local anaesthetic (lignocaine) is injected at the wrist. A small needle punctures the radial artery, through which a thin guidewire and then a plastic sheath (introducer) is placed. You will feel mild pressure but no sharp pain at this point.
Catheter Advancement to the Heart
A thin, flexible catheter (approximately 2–2.5 mm in diameter) is gently advanced through the sheath, along the arterial system, and up into the aorta to the heart. There are no pain nerves inside the blood vessels, so you will feel no pain during this step.
Contrast Injection and X-ray Imaging
The catheter tip is engaged at the opening of each coronary artery. A small volume of contrast dye is injected while X-ray images are captured in multiple projections (angles). When contrast is injected, you may feel a brief warm, flushing sensation — this is normal and harmless and passes within seconds.
Left Ventriculogram (If Required)
In some cases, the cardiologist will also inject contrast into the left ventricle (the main pumping chamber) to assess its function and contractility. This produces a more intense warm flush sensation, which is temporary.
Sheath Removal and Haemostasis
Once the imaging is complete, the catheter and sheath are removed. For radial access, a small patent haemostasis device (wristband) is applied to compress the puncture site. You will wear this for 2–3 hours. There are no stitches required.
Recovery and Results Discussion
After a 2–4 hour observation period in the recovery area, your cardiologist will discuss the angiography findings with you and your family. If significant blockages are found, the treatment plan — medical management, angioplasty, or bypass surgery — will be explained.
Understanding Your Angiography Results
How stenosis severity is measured and what each level of blockage means for treatment.
FFR (Fractional Flow Reserve) is a wire-based test performed during angiography to measure the functional significance of an intermediate stenosis (50–70%). A lesion with FFR ≤ 0.80 is confirmed haemodynamically significant and warrants treatment. The FAME trial demonstrated that FFR-guided PCI reduces major adverse cardiac events by 28% compared to angiography-guided PCI alone.
Benefits and Risks of Coronary Angiography
A balanced, evidence-based view of the procedure's safety and effectiveness.
Core Clinical Benefits
- Definitive diagnosis — eliminates uncertainty from non-invasive tests
- Maps the exact anatomy of every coronary artery
- Enables immediate treatment (ad-hoc PCI) if indicated
- Essential for surgical planning (CABG decisions)
- Assesses left ventricular function
- Short procedure, local anaesthesia, same-day discharge possible
Potential Risks & Incidence
- Bruising/haematoma at wrist: <2% with radial access
- Contrast allergy: 0.1–0.5% (pre-medicated if at risk)
- Contrast nephropathy: <1% in normal kidney function
- Stroke or MI: <0.05% at experienced centres
- Coronary artery dissection: extremely rare (<0.01%)
- Death: <0.05% (lower than risk of untreated CAD)
Recovery: What to Expect After
What happens after your angiography — from the recovery bay to the first 48 hours at home.
In the Hospital (First 4–6 Hours)
- You will rest in a monitored recovery bay for 2–4 hours.
- A haemostasis band is worn on the wrist for 2–3 hours after radial access; a trained nurse will gradually deflate and remove it.
- You can sit up, eat, and drink normally within 1–2 hours.
- Your cardiologist will visit to explain the angiography findings and discuss the treatment plan.
- Most patients undergoing elective diagnostic-only angiography are discharged on the same day.
At Home (First 24–48 Hours)
- Avoid driving for 24 hours after the procedure due to residual sedation.
- Keep the wrist dry for 24 hours. Avoid heavy lifting with the access arm for 48 hours.
- Watch for warning signs: increasing wrist pain, swelling above or below the bandage, bleeding, chest pain, or breathlessness — call 97695 17636 or visit the emergency department immediately.
- Drink 1.5–2 litres of water over the first 24 hours to help the kidneys flush out contrast dye.
- Resume normal activities and medications as directed by your cardiologist.
Landmark Clinical Evidence
Key trials and meta-analyses supporting radial access coronary angiography.
Radial access reduces major bleeding complications by 73% compared to femoral access
n = 7,021 patients. N Engl J Med 2011;365:774–784The landmark RIVAL trial (2011, New England Journal of Medicine, n = 7,021 patients) established that radial access angiography reduces major bleeding complications at the access site by 73% compared to femoral access. Subsequent meta-analyses involving over 24,000 patients have consistently confirmed this advantage, particularly in patients receiving anticoagulant and antiplatelet therapy.
Frequently Asked Questions
The most common concerns raised by patients before coronary angiography — each answer is self-contained and evidence-based.
Coronary angiography is performed under local anaesthesia at the wrist with mild intravenous sedation. Most patients experience only mild pressure at the catheter insertion site and no pain during the procedure. There are no pain-sensing nerves inside blood vessels or the coronary arteries, so the passage of the catheter is painless. When contrast dye is injected, a brief warm, flushing sensation is common — this is temporary, lasting only a few seconds, and is harmless.
The coronary angiography procedure itself typically takes 30 to 60 minutes. Complex cases or those requiring additional functional testing (FFR, IVUS) may take longer. Including pre-procedure preparation and post-procedure observation, patients should plan for approximately 4 to 6 hours at the hospital. In most cases of elective diagnostic angiography performed via the radial approach, same-day discharge is routine.
The radial approach is a technique where the catheter is inserted through the radial artery at the wrist rather than the femoral artery at the groin. The landmark RIVAL trial (NEJM, n = 7,021) established that radial access reduces major bleeding complications by 73% compared to femoral access. Patients can sit up and walk immediately after the procedure, and same-day discharge is routinely possible. Radial access is the preferred approach at Heartwise Cardiology wherever anatomically feasible.
Coronary angiography is a safe, routinely performed procedure with a major complication rate of less than 0.1% in experienced interventional centres (ESC Guidelines 2023). The risk of stroke or heart attack related to the procedure is less than 0.05%. Minor complications — such as bruising at the access site — occur in under 2% of cases with radial access. The procedure is performed in a dedicated Cath Lab with full resuscitation equipment and a trained cardiac team present throughout.
Angiography results are reported as percentage stenosis — the degree of narrowing in each coronary artery. Blockages below 50% are generally non-significant and managed with medications. Stenosis between 50–70% is intermediate and may require additional functional testing (FFR) to decide on treatment. Stenosis above 70% is clinically significant and typically warrants angioplasty with stenting. Total occlusions (100% blockage) are treated urgently. Your cardiologist will explain your specific results in detail after the procedure.
Fast for 4 to 6 hours before the procedure. Inform your cardiologist of all medications — particularly blood thinners (aspirin, clopidogrel, warfarin) and diabetic medication (metformin should be stopped 24–48 hours prior). Blood tests, an ECG, and kidney function tests (creatinine) will be done beforehand. Arrange a companion who can drive you home, as you will not be permitted to drive for 24 hours. Leave jewellery at home and wear comfortable, loose-fitting clothing.
If the angiography reveals significant coronary artery disease, your interventional cardiologist will discuss three possible treatment paths: optimised medical therapy alone (for mild disease), coronary angioplasty and stenting (PCI — often performed in the same sitting as the angiogram, known as an ad-hoc procedure), or coronary artery bypass surgery (CABG — recommended for complex multi-vessel disease or left main artery involvement). The best option depends on the number, location, and severity of blockages as well as your overall health.
Coronary angiography is classified as a listed medical procedure and is covered under most Indian health insurance policies, including CGHS (Central Government Health Scheme), ECHS (Ex-Servicemen Contributory Health Scheme), and Ayushman Bharat Pradhan Mantri Jan Oyoana (PM-JAY). Most private health insurers (Star Health, New India, ICICI Lombard, HDFC Ergo) also cover the procedure. Pre-authorisation from your insurer and an original cardiologist referral letter are typically required. Contact Heartwise Cardiology on 97695 17636 for insurance guidance.
“Precision in structural interventions. Excellence in clinical outcomes.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management at Heartwise Cardiology Clinic, Vashi.
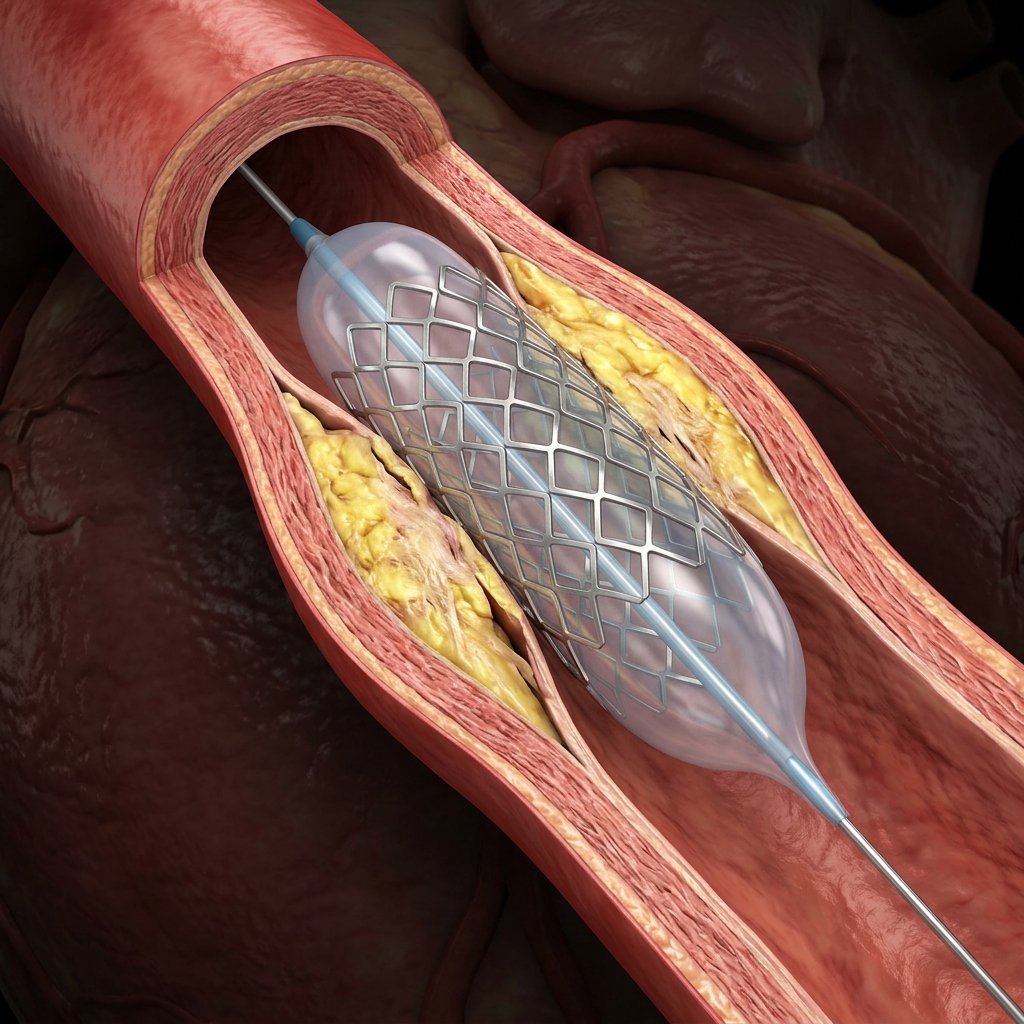
Coronary Angioplasty & Stenting
Balloon angioplasty and drug-eluting stent implantation following angiography.

2D Echocardiography
Non-invasive cardiac ultrasound for structural and functional assessment.

Treadmill Stress Test
Exercise ECG to detect coronary ischaemia before angiography.
Coronary Artery Disease
Comprehensive CAD management including medical therapy and revascularisation.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.