
MitraClip Procedure Mitral Valve Repair Without Surgery
A minimally invasive transcatheter edge-to-edge repair (TEER) for severe Mitral Regurgitation (MR). Clinically proven to reduce heart failure hospitalisations by 47% and lower mortality by 38% under Kokilaben Hospital's elite structural heart program.
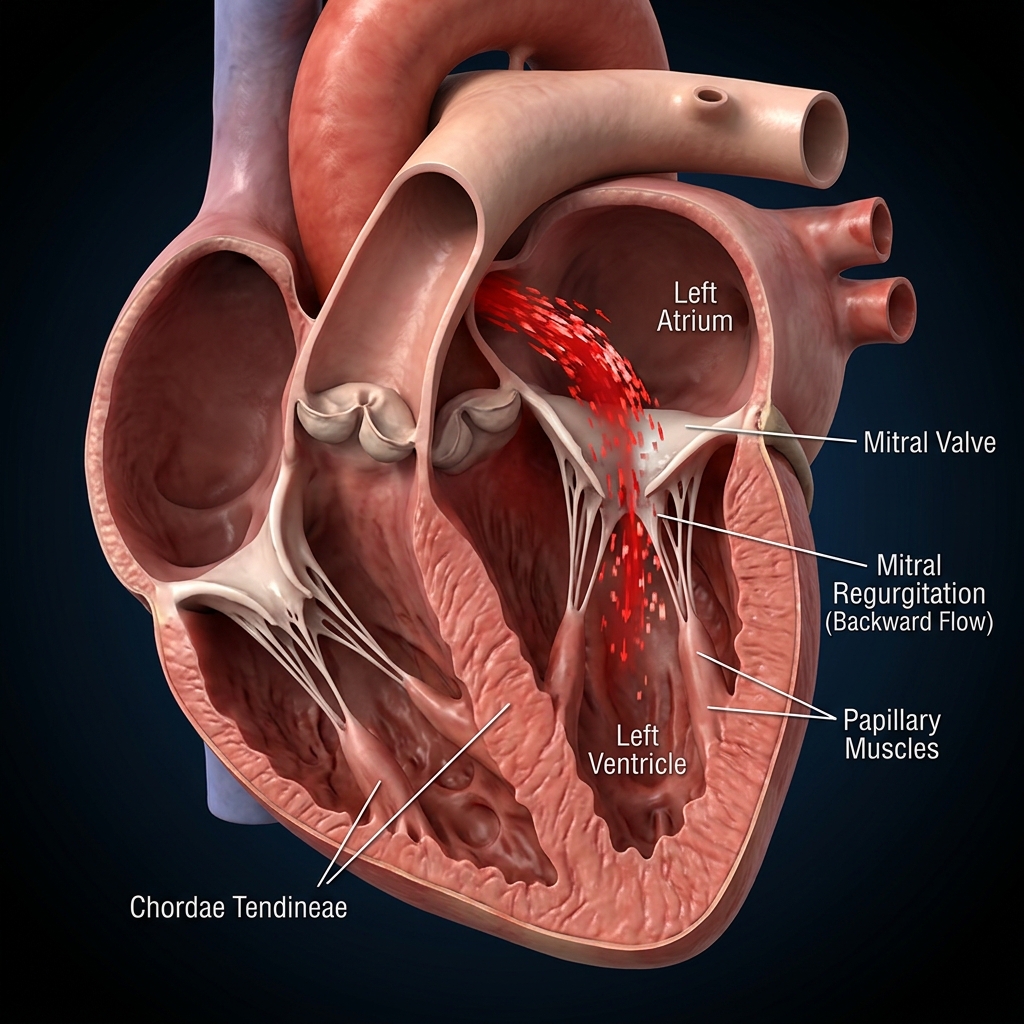
Understanding Mitral Regurgitation (MR)
An evidence-based overview of mitral valve leakage, chambers enlargement, and functional volume burden.
Mitral regurgitation (MR) — also called mitral insufficiency or mitral incompetence — is a condition in which the mitral valve, located between the left atrium and left ventricle, fails to close completely during each heartbeat. This allows blood to flow backwards (regurgitate) from the ventricle into the atrium with each contraction, rather than forward into the aorta. The result is a volume overload on the left ventricle — it must pump the same blood twice — leading to progressive left ventricular dilation and, ultimately, heart failure. Severe mitral regurgitation is the most common indication for mitral valve intervention worldwide. MR is graded from 1+ (mild, trace) to 4+ (severe) based on echocardiographic assessment of the regurgitant jet area, vena contracta width, effective regurgitant orifice area (EROA), and regurgitant volume. MitraClip is indicated for symptomatic MR Grade 3+ or 4+ (significant or severe).
Trivial/Mild — Small jet on echo. No haemodynamic significance.
No treatment neededModerate — Moderate jet. Serial surveillance.
Optimise risk factorsSignificant — Significant volume overload. Symptoms developing.
Consider interventionSevere — Severe regurgitation. Heart failure.
Intervention indicatedThe Alfieri Stitch & TEER Technique
How the native leaflets are grasped and held together using real-time TOE guidance.
Anaesthesia & TOE Preparation
General anaesthesia is administered. A transoesophageal echo (TOE) probe is placed for continuous real-time cardiac imaging throughout the procedure. Femoral venous access is established.
Transseptal Puncture
A catheter is advanced from the right femoral vein to the right atrium. Under TOE and fluoroscopic guidance, a needle punctures the interatrial septum — creating a small controlled hole that provides access to the left heart. The precise puncture location is critical for optimal clip delivery trajectory.
Steerable Guide Catheter Delivery
The steerable guide catheter and clip delivery system are advanced through the transseptal opening into the left atrium, then directed towards the mitral valve using a combination of TOE imaging and fluoroscopy. The system can be steered in multiple planes to optimise approach angle.
Clip Positioning & Leaflet Grasping
The open clip is advanced through the mitral valve into the left ventricle. It is then retracted back across the valve, grasping both the anterior and posterior leaflets simultaneously with its fine wire grippers. TOE confirms both leaflets are properly engaged in the clip before it is closed. This is the most technically demanding step — accurate leaflet capture directly determines the degree of MR reduction.
MR Assessment & Additional Clips
TOE colour Doppler immediately confirms the degree of MR reduction after the clip is closed. If residual MR ≥ Grade 2+ is present at the same coaptation zone or a different segment, additional clips are deployed in sequence. The clip can be reopened and repositioned if needed before final release.
Clip Release & Recovery
Once satisfactory MR reduction (target ≤ Grade 2+) and adequate mitral valve area (≥1.5 cm² per clip) are confirmed, the clip is released from the delivery system. Vascular closure is performed. Patient is transferred to Cardiac ICU for 12–24 hours then ward. Discharge typically day 2.
COAPT vs MITRA-FR: Trial Comparison
Understanding the vital concept of proportionate vs disproportionate functional mitral regurgitation.
MitraClip reduced HF hospitalisation by 47% and all-cause mortality by 38% at 2 years vs optimal medical therapy in patients with HF and severe functional MR. Enrolled disproportionate MR phenotype.
Stone GW et al. NEJM 2018;379:2307–2318No significant difference in death or unplanned hospitalisations at 12 months between MitraClip and medical therapy in patients with proportionate functional MR — MR was a consequence of LV dilation, not an independent driver.
Obadia JF et al. NEJM 2018;379:2297–2306MitraClip was safer than surgery but produced more residual MR (Grade 2+ at 1 year: 20% vs 1%). Established the role of TEER for primary MR in high-risk surgical patients.
Feldman T et al. NEJM 2011;364:1395–1406TEER works when the leaking valve is disproportionately severe compared to the heart enlargement. In these patients, fixing the valve relieves the heart. This patient selection standard is carefully evaluated by our Heart Team.
Candidate Criteria Checklist
How we determine suitability for transcatheter edge-to-edge valve repair.
Favourable vs Unfavourable Profiles
Detailed breakdown of patient characteristics that predict MitraClip response.
Favourable Profile
- Severe functional MR (Grade 3+/4+) with symptoms despite optimised medications
- Effective Regurgitant Orifice Area (EROA) ≥0.20 cm² (COAPT Phenotype)
- Left Ventricular End-Systolic Diameter (LVESD) ≤70 mm
- Mitral valve area ≥4.0 cm² (accommodates clips safely)
- High surgical risk or sternotomy contraindications
Less Favourable
- Primary MR in surgically fit patients (open repair remains gold standard)
- Severe LV dilation (LVESD >70 mm - proportionate MR)
- Mitral valve area <4.0 cm² (risk of causing valve narrowing)
- Coaptation gap >10 mm or severely calcified leaflets
- Active infective endocarditis or acute sepsis
Benefits, Risks & Recovery Timeline
Detailed risk evaluation and the expected recovery process without sternotomy.
Core Clinical Benefits
- No chest wound or heart-lung bypass required
- Relief of shortness of breath within days
- Reduced heart failure hospitalisations
- 2 to 3 days hospital stay with rapid mobilization
Potential Risks & Incidence
- Residual leak: 10-15%, managed with additional clips
- Transseptal complications: rare, <1%
- Partial clip detachment or embolisation: <0.5%
- Access site hematoma or bleeding: <1%
Frequently Asked Questions
Detailed, peer-reviewed answers to the most common patient concerns regarding stenting and long-term care.
MitraClip is a transcatheter edge-to-edge repair (TEER) technique that places a small clip on the mitral valve leaflets via a catheter through the femoral vein — without opening the chest. The clip grasps and approximates the anterior and posterior leaflets, reducing the degree of backwards blood leakage through the valve. The procedure is performed under general anaesthesia with real-time transoesophageal echocardiographic (TOE) guidance. Hospital stay is 2–3 days. Most patients experience significant improvement in breathlessness within days.
In carefully selected heart failure patients with severe functional mitral regurgitation, MitraClip reduces the volume of blood leaking backwards through the mitral valve — decreasing the volume burden on the left ventricle and reducing pulmonary congestion. The COAPT trial (NEJM 2018, n=614) demonstrated MitraClip reduced heart failure hospitalisation by 47% and all-cause mortality by 38% at 2 years compared to optimal medical therapy alone. These results directly updated the 2021 ESC Heart Failure Guidelines, which now give MitraClip a Class IIa recommendation for appropriate patients.
Primary (degenerative) mitral regurgitation occurs when the mitral valve itself is structurally abnormal — most commonly due to mitral valve prolapse, chordal rupture, or rheumatic disease. Secondary (functional) mitral regurgitation occurs when the valve is structurally normal but fails to close because the left ventricle is enlarged by heart failure, pulling the valve leaflets apart. The distinction matters for MitraClip: the strongest evidence is in secondary/functional MR in heart failure (COAPT trial). For primary MR in surgically fit patients, open surgical repair is preferred.
For primary (degenerative) MR in a surgically fit patient, open-heart surgical valve repair remains the gold standard — it achieves more complete anatomical correction. The EVEREST II trial showed MitraClip is safer but produces more residual MR compared to surgery. For secondary (functional) MR in heart failure patients at high surgical risk, MitraClip is preferred — the COAPT trial shows clear clinical benefit and surgery in this population carries prohibitive mortality. The Heart Team evaluates each patient individually — there is no universal answer.
After MitraClip, patients spend 12–24 hours in the Cardiac ICU, then are transferred to the ward. Most are discharged on day 2 or 3. No sternotomy means no chest wound — recovery is dramatically faster than surgical repair. Light activity is permitted from day 1; driving is allowed after 1 week. Most patients notice significant improvement in breathlessness within days. Follow-up echocardiogram at 1 month, 3 months, and annually. Heart failure medications (GDMT) must be continued and optimised — MitraClip works alongside medical therapy, not instead of it.
COAPT enrolled patients with 'disproportionate' functional MR — their MR severity (EROA ≥0.20 cm²) was larger than expected for their degree of LV dilation. In these patients, the MR is a significant independent driver of heart failure deterioration, and reducing it with MitraClip produces major benefit. MITRA-FR enrolled patients with 'proportionate' MR — their MR was largely a consequence of advanced LV dilation, not an independent driver. In these patients, fixing the valve does not address the underlying problem. This patient selection distinction is now the most critical determinant of who will benefit from MitraClip.
MitraClip vs Surgical Mitral Valve Repair
Head-to-head comparison of transcatheter edge-to-edge repair versus open surgical mitral valve repair.
Pre-MitraClip Workup & Preparation
Essential investigations and patient optimisation before transcatheter mitral valve repair.
Recovery After MitraClip
Expected recovery trajectory after transcatheter edge-to-edge mitral valve repair.
In Hospital (Days 1–3)
- ICU monitoring 12–24 hours post-procedure with continuous haemodynamics
- TOE next day to confirm clip position, assess residual MR, and rule out complications
- Mobilise from day 1; chest physiotherapy encouraged
- Antibiotic prophylaxis for 24 hours; continue GDMT
- Discharge typically day 2–3 with clear follow-up plan
First Month After Discharge
- Light activity from day 1; no heavy lifting for 2 weeks
- Wound care: keep femoral access site dry for 48 hours
- Echocardiogram at 1 month: assess residual MR, LV reverse remodelling
- Heart failure medications (GDMT) must be continued and optimised
- Driving permitted after 1 week
Long-Term Follow-Up
- Clinical + echo at 1 month, 3 months, 6 months, then annually
- Lifelong HF medication optimisation essential
- Endocarditis prophylaxis for dental procedures in first 6 months
- Residual MR progression: monitor annually; re-intervention if symptomatic
Post-MitraClip Results Interpretation
Key echocardiographic and clinical parameters for assessing MitraClip procedural success.
“Precision in structural interventions. Excellence in clinical outcomes.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management at Heartwise Cardiology Clinic, Vashi.

2D Echocardiography
Detailed echo assessment of MR severity and mitral valve anatomy.
Coronary Angiography
Pre-MitraClip coronary assessment to rule out significant CAD.

Heart Failure
GDMT optimisation for secondary MR in heart failure patients.
Mitral Valve Disease
Comprehensive mitral valve disease evaluation and management.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.