High-Risk & Complex Angioplasty
IVL · Rotablation · CTO · Left Main · Bifurcation · Multi-Vessel. High-risk complex coronary angioplasty — also called CHIP (Complex High-risk Indicated Procedures) — refers to percutaneous coronary interventions that carry elevated procedural risk due to patient clinical factors or complex anatomy. Dr. Amit Singh, FACC performs the full spectrum of complex PCI at Kokilaben Dhirubhai Ambani Hospital, Koperkhairne, Navi Mumbai.
What Makes an Angioplasty High-Risk or Complex?
Not all coronary blockages are equal in difficulty. Complexity arises from patient overall clinical condition and the coronary anatomy itself.
Were you told bypass surgery is your only option? Advances in interventional techniques — including Intravascular Lithotripsy (IVL), Rotational Atherectomy, and retrograde Chronic Total Occlusion (CTO) wires — have dramatically expanded what is safely treatable via stenting. Dr. Amit Singh offers experienced, transparent consultations and second opinions for high-risk complex cases.
The SYNTAX Score: PCI vs Bypass Decision
The primary anatomical scoring system that quantifies coronary disease complexity to guide clinical revascularisation choices.
Clinical scenarios where PCI is preferred: Low/intermediate SYNTAX left main disease — EXCEL trial: comparable 5-year outcomes to CABG. High surgical risk (frailty, CKD, prior CABG) — avoids open-chest risks; faster recovery. Patient refuses surgery — complex PCI may be viable alternative after full counselling. Calcified lesions with low SYNTAX — IVL/rotablation enables successful stenting without surgery. CTO in single-vessel disease — successful CTO PCI eliminates need for surgery in selected cases. Re-do CABG scenario (patent grafts) — native vessel or graft PCI avoids high re-operative mortality.
The Advanced Techniques Dr. Amit Singh Uses
Each of these advanced interventions extends the reach of coronary stenting into territory previously considered untreatable or requiring bypass.
Intravascular Lithotripsy (IVL)
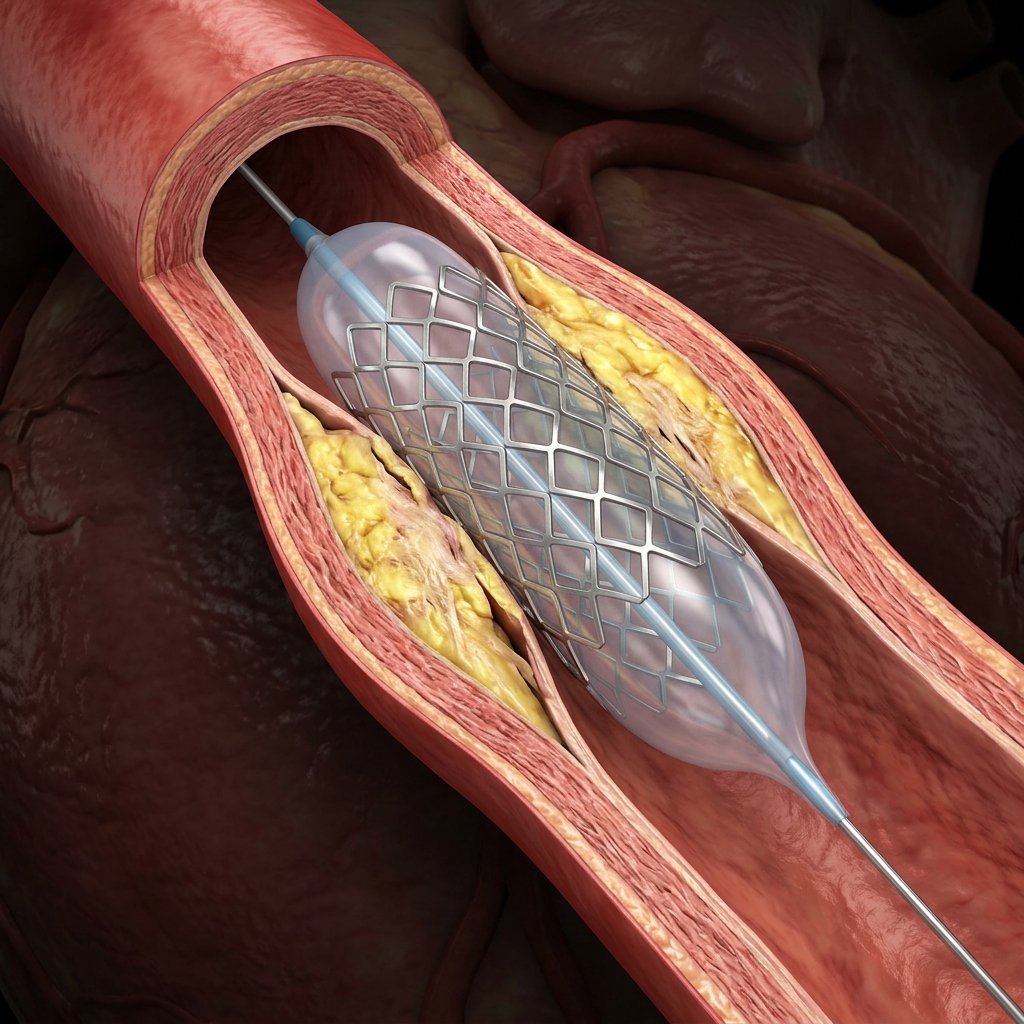
01IVL uses pulsatile sonic pressure waves — the same physics as kidney stone lithotripsy — delivered from inside the coronary artery to fracture both superficial and deep calcium deposits without damaging the vessel wall or surrounding tissue. A specialised balloon catheter containing miniature lithotripters is positioned at the calcified segment. Each pulse generates a focused shockwave that cracks the calcium circumferentially, dramatically softening the artery and enabling optimal stent expansion at low balloon pressures. IVL has transformed the treatment of severely calcified coronary disease — lesions that previously required rotational atherectomy or were referred for bypass surgery can now be treated safely and predictably.
IVL achieved optimal stent expansion (<50% residual stenosis with full expansion) in over 70% of severely calcified lesions. Major adverse cardiac events at 30 days: 7.6%. Procedure success: 92.4%.
Rotational Atherectomy (Rotablation)
02Rotational atherectomy uses a high-speed (140,000–180,000 rpm) diamond-coated burr advanced over a coronary guidewire to ablate calcified plaque. The differentially cutting mechanism ablates hard calcified tissue while deflecting the softer, elastic normal vessel wall — converting calcium into microparticles smaller than 10 µm that are safely cleared by the reticuloendothelial system. Rotablation changes vessel compliance — converting a rigid, calcified tube into a more distensible segment that accepts a stent. It is particularly used for lesions with concentric calcium that prevents adequate pre-dilation or stent delivery.
IVUS-guided rotablation + stenting achieved optimal IVUS expansion criteria in 76% of cases versus 55% with angiography guidance alone.
Bifurcation PCI
03Bifurcation lesions — blockages at arterial branch points — occur in approximately 15–20% of all PCI cases and carry higher procedural complication rates and restenosis risk than non-bifurcation disease. The challenge is maintaining flow in both the main vessel and the side branch simultaneously. A provisional one-stent strategy (treating the main vessel first, with selective side-branch stenting only if needed) is preferred for most bifurcations. For complex true bifurcations involving a large side branch, a two-stent technique — DK-Crush (demonstrated superior in the DKCRUSH-V trial) or Culotte — is employed. OCT guidance is used to confirm optimal stent apposition and detect side-branch jailing after kissing balloon inflation.
OCT-guided bifurcation PCI reduced 2-year MACE by 21% relative reduction versus angiography-guided bifurcation PCI.
Left Main Coronary Artery PCI
04The left main coronary artery — which supplies 70–80% of the left ventricular myocardium — was historically treated exclusively by bypass surgery. The EXCEL (2016) and NOBLE (2016) randomised trials established left main PCI as a guideline-supported alternative to CABG in patients with low-to-intermediate SYNTAX scores, with 5-year outcomes comparable to surgery. IVUS guidance is mandatory for left main PCI — the true vessel diameter (frequently 4–5 mm) is consistently underestimated by angiography alone, and stent underexpansion in the left main is the most common cause of failure. Post-stent OCT or IVUS confirmation of full expansion, complete apposition, and absence of edge dissection is performed in every case. All left main PCI cases at Heartwise Cardiology are discussed in a cardiac surgical team context before proceeding.
Left main PCI vs CABG: Death/stroke/MI at 5 years — 22.0% vs 19.2%. Comparable outcomes in low-intermediate SYNTAX score patients.
Chronic Total Occlusion (CTO) PCI
05A Chronic Total Occlusion (CTO) is a coronary artery that has been completely blocked (100% stenosis) for more than 3 months. CTO PCI is the most technically challenging procedure in interventional cardiology — it uses specialised antegrade and retrograde wire crossing techniques, dedicated CTO guidewires, and microcatheters to navigate through the occluded segment and restore blood flow. In experienced, high-volume CTO operators, procedural success rates exceed 85–90%. Successful CTO PCI relieves angina, reduces ischaemia, and in patients with viable but hibernating myocardium, may improve left ventricular function.
Development and Validation of a Scoring System for Predicting CTO PCI Success — procedural success >85% in high-volume operators.
Multi-Vessel FFR-Guided PCI
06In patients with blockages in two or three coronary arteries simultaneously, a critical decision must be made: treat all lesions, or only the most functionally significant ones? Treating anatomically significant but haemodynamically non-significant stenoses adds procedural risk, stent material, and DAPT duration without clinical benefit. The FAME 2 trial established that FFR-guided PCI — treating only stenoses with FFR ≤ 0.80 — is superior to both angiography-guided PCI and medical therapy alone for haemodynamically significant lesions. In multi-vessel disease, FFR guidance determines which lesions truly require stenting, resulting in fewer stents, shorter DAPT duration, and equivalent or better clinical outcomes than treating all anatomical stenoses. A staged approach — treating the culprit vessel first, then returning for other significant vessels in a separate session 2–6 weeks later — is generally preferred over single-session multi-vessel PCI.
FFR-guided PCI superior to medical therapy for haemodynamically significant lesions. Composite primary endpoint: 4.3% vs 12.7% at 2 years.
Key Trials in Complex PCI
Landmark randomised trials that define the evidence base for complex and high-risk coronary interventions.
Left main PCI vs CABG — comparable outcomes at 5 years in low-intermediate SYNTAX score patients.
Death/stroke/MI at 5 years: PCI 22.0% vs CABG 19.2%FFR-guided PCI superior to medical therapy alone for haemodynamically significant coronary lesions.
Composite primary endpoint at 2 yearsOCT-guided bifurcation PCI reduces 2-year MACE versus angiography-guided PCI.
Relative reduction in 2-year MACE with OCT guidancePre-Procedure Workup for Complex PCI
Critical pre-procedure checklist for safe and effective complex coronary intervention.
Benefits & Risks of Complex PCI
A scientific, transparent perspective on procedural outcomes and safety of high-risk coronary interventions.
Core Clinical Benefits
- Avoids open-chest surgery in patients with prohibitively high surgical risk
- Completes revascularisation in anatomy previously deemed untreatable percutaneously
- Preserves left ventricular function by restoring flow to chronically occluded territories
- Haemodynamic support enables treatment in patients with severely reduced EF
- Same-day ambulation and short hospital stay versus CABG
- Can be staged across multiple sessions to reduce contrast and radiation burden
Potential Risks & Incidence
- Periprocedural MI: 3–5% in complex PCI vs <1% in routine PCI
- Contrast nephropathy: 5–15% in CKD patients; meticulous prevention required
- Stroke: 0.5–1% in left main or multi-vessel complex PCI
- Coronary perforation: 1–3% in CTO PCI; usually manageable with covered stent
- Emergent CABG: <1% with modern techniques but must be consented
- Radiation injury: Possible with prolonged fluoroscopy (>60 min)
- Death: 1–3% in high-risk elective complex PCI; higher in emergency setting
Recovery After Complex PCI
Structured recovery timeline and follow-up protocol after high-risk complex coronary intervention.
In-Hospital Monitoring (24–48 hours)
- ICU monitoring for first 12–24 hours after complex PCI
- ECG and cardiac enzymes at 6, 12, and 24 hours to rule out periprocedural MI
- Echocardiogram before discharge to confirm no new wall motion abnormality
- DAPT continued uninterrupted; IV fluids for contrast nephropathy prevention
- Wrist haemostasis band removed at 2–3 hours; assess access site before discharge
First Month After Discharge
- Strict DAPT adherence — aspirin + ticagrelor or prasugrel for minimum 12 months
- Wound care: keep wrist/groin dry for 48 hours; report any swelling or bruising
- Activity: light walking only for first week; no heavy lifting (>5 kg) for 2 weeks
- Cardiac rehabilitation referral if LVEF <40% or deconditioned
- Follow-up at 1 month: clinical review, ECG, echo, basic blood work
Long-Term Follow-Up
- Continue optimal medical therapy: statin, beta-blocker, ACEi/ARB, DAPT
- Stress test or CT coronary angiogram at 6–12 months if symptoms recur
- Annual cardiology review with risk factor optimisation
- DAPT duration: minimum 12 months; consider extended if high ischaemic risk
Post-Complex PCI Assessment
Interpretation of procedural results after high-risk complex coronary intervention.
Frequently Asked Questions
Detailed, peer-reviewed answers to the most common patient concerns regarding stenting and complex care.
A coronary angioplasty is classified as high-risk when patient clinical factors — severely reduced ejection fraction (<35%), chronic kidney disease, diabetes, prior CABG, advanced age — or coronary anatomy factors — calcification, CTO, left main disease, bifurcation, three-vessel disease with high SYNTAX score — increase procedural complexity and risk above routine PCI. These cases require specialist training, dedicated equipment (IVL, rotablation, CTO wires, IVUS/OCT), and experienced judgment. They should not be attempted in non-specialist settings.
Intravascular Lithotripsy (IVL) uses pulsatile sonic pressure waves — delivered from inside the coronary artery via a specialised balloon catheter — to fracture both superficial and deep calcium deposits without damaging the vessel wall. This softens severely calcified arteries, allowing optimal stent expansion. The DISRUPT CAD IV trial (NEJM 2024) demonstrated IVL achieves optimal stent expansion in over 70% of severely calcified lesions — lesions that previously required rotational atherectomy or surgical referral — with a major complication rate of less than 2%.
Rotational atherectomy — commonly called Rotablation — uses a high-speed (up to 180,000 rpm) diamond-tipped burr to ablate calcified plaque inside the coronary artery, converting it into microparticles smaller than red blood cells that are safely cleared by the body. The differential cutting mechanism ablates hard calcium while deflecting the softer vessel wall. This changes vessel compliance, enabling stent delivery and expansion in arteries that cannot be adequately dilated with standard balloons. It is used in approximately 5–8% of PCI procedures at high-volume interventional centres.
Yes — and it costs nothing to get one. Advances in complex PCI — intravascular lithotripsy, rotational atherectomy, CTO retrograde crossing techniques, IVUS-guided left main stenting, and haemodynamic support devices — have substantially expanded what is safely treatable with angioplasty versus what requires open-heart surgery. Many patients told stenting is impossible for heavily calcified arteries or chronic total occlusions may be candidates for complex PCI at a specialist centre. Dr. Amit Singh, FACC offers second opinion consultations at Heartwise Cardiology, Vashi, Navi Mumbai. Call 9769517636.
A chronic total occlusion (CTO) is a coronary artery that has been completely blocked for more than 3 months. Standard guidewires cannot cross a CTO — it requires dedicated CTO guidewires, microcatheters, and specialised crossing strategies (antegrade wire escalation, antegrade dissection re-entry, or retrograde crossing via collateral channels). In experienced CTO operators, procedural success exceeds 85–90%. Successful CTO PCI relieves angina, reduces ischaemia, and may improve ventricular function in patients with viable hibernating myocardium.
Yes — in carefully selected patients. The left main coronary artery supplies 70–80% of the heart. The EXCEL trial (NEJM 2016/2019, 5-year follow-up) demonstrated left main PCI achieves outcomes comparable to bypass surgery in patients with low-to-intermediate SYNTAX scores. IVUS guidance is mandatory — the true left main diameter is consistently underestimated on angiography, and stent underexpansion is the leading cause of failure. All left main PCI cases are discussed in a multidisciplinary cardiac team context before proceeding.
“Precision in structural interventions. Excellence in clinical outcomes.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management at Heartwise Cardiology Clinic, Vashi.
Coronary Angiography
Diagnostic angiography with IVUS, OCT, and FFR for complex lesions.
Coronary Angioplasty & Stenting
Standard PCI with drug-eluting stents for less complex disease.

2D Echocardiography
LV function, wall motion, and valve assessment pre and post procedure.

Heart Failure
Post-MI heart failure management and ischaemic cardiomyopathy care.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.