Mitral Valve Disease
Mitral valve disease takes two principal forms: mitral regurgitation (MR) — the valve leaks backwards — and mitral stenosis (MS) — the valve is narrowed and obstructs forward flow. Learn about echo grading, MitraClip repair, and balloon mitral valvotomy.
What Is Mitral Valve Disease?
The mitral valve coordinates blood flow from the left atrium into the left ventricle, operating under intense pressure loads.
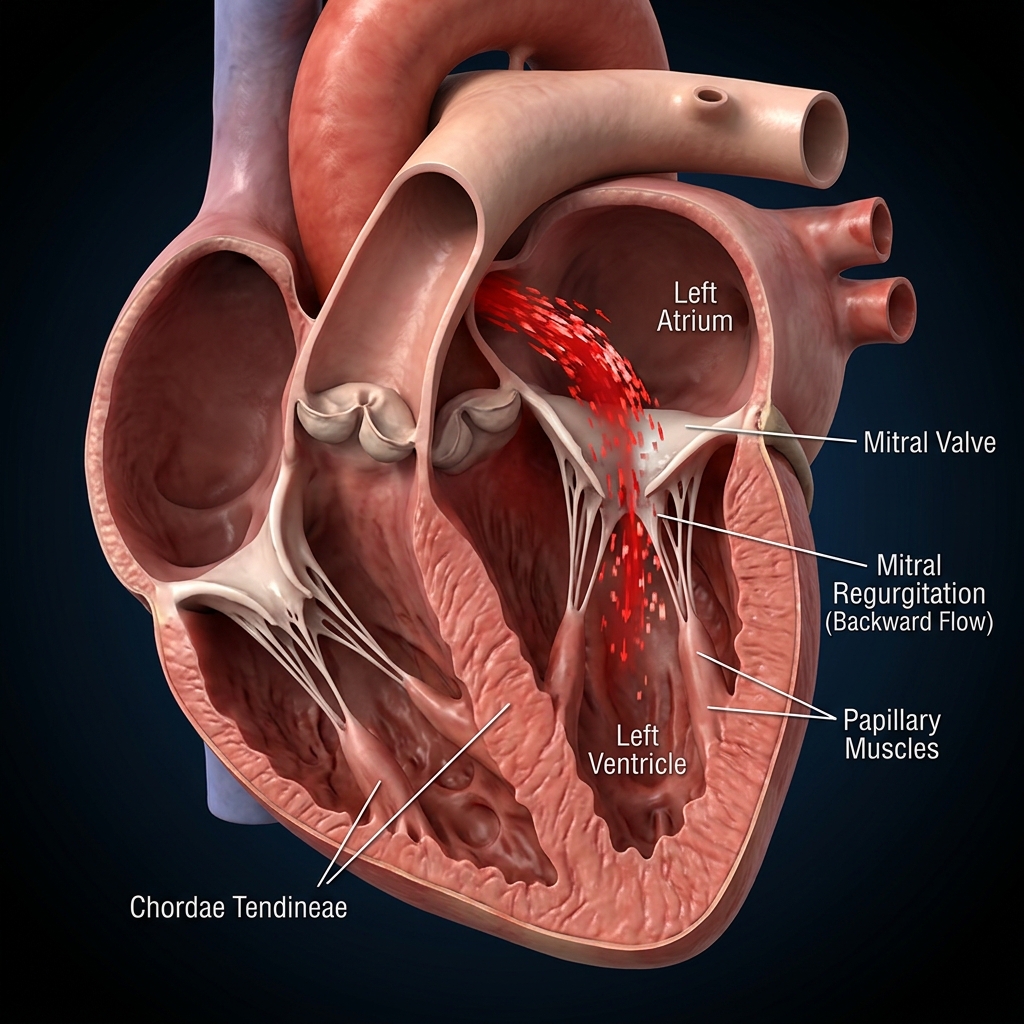
Mitral regurgitation (MR) represents a leaking valve where blood backs up into the atrium during contraction. Mitral stenosis (MS) describes a narrowed valve that blocks forward flow. Comprehensive Doppler echo scans are standard to grade severity and determine repair timing.
Causes & Risk Factors for Mitral Valve Disease
MR and MS have distinct underlying causes and risk factors.
Primary Degenerative MR
Mitral Valve Prolapse (MVP), flail leaflets, chordal rupture, or infective endocarditis physically damage the leaflets. Valve repair surgery is highly preferred over replacement.
Secondary Functional MR
Dilated or ischaemic cardiomyopathies enlarge the left ventricle, pulling normal leaflets apart. Optimising SGLT2i and ARNi therapies is primary.
Rheumatic Heart Disease (MS)
In India, the dominant cause of mitral stenosis is rheumatic heart disease — valve damage following childhood streptococcal throat infection and rheumatic fever.
Infective Endocarditis
Bacterial infection of the mitral valve causes leaflet destruction, perforation, or abscess formation. Leads to acute severe MR requiring urgent surgery.
Ischaemic MR
Prior MI causing papillary muscle dysfunction or LV remodelling. The valve is structurally normal but the supporting apparatus is damaged.
Congenital & Connective Tissue Disease
MVP with myxomatous degeneration, Marfan syndrome, Ehlers-Danlos syndrome, and cleft mitral valve are less common causes of MR.
Types & Severity of Mitral Valve Disease
MR and MS are graded by echocardiographic parameters.
Signs & Symptoms of Mitral Valve Disease
Symptoms depend on the severity and type of valve lesion.
Breathlessness on Exertion
The most common symptom. Reduced forward flow in MS or volume overload in MR causes effort intolerance and dyspnoea.
Palpitations
LA enlargement from MR or MS predisposes to atrial fibrillation. AF causes palpitations and further reduces cardiac output.
Fatigue & Reduced Capacity
Reduced cardiac output from the valve lesion causes profound fatigue. Patients often limit activities unconsciously.
Heart Failure Symptoms
Advanced disease causes orthopnoea, PND, peripheral oedema, and pulmonary congestion. Indicates need for urgent intervention.
How Is Mitral Valve Disease Diagnosed?
Doppler echocardiography is the cornerstone of diagnosis and severity assessment.
Transthoracic Echocardiography (TTE)
Assesses valve morphology, jet characteristics, MVA (pressure half-time, planimetry), LA size, LV function, and pulmonary pressure. Grades MR and MS severity.
Transoesophageal Echo (TOE/TOE)
Higher resolution images of the mitral apparatus. Essential before MitraClip, PBMV, or surgical repair. Defines MR mechanism (Carpentier classification).
Wilkins Echocardiographic Score (MS)
Leaflet mobility, thickening, subvalvular fusion, and calcification scored 0–4 each. Total score ≤8 predicts excellent PBMV outcome.
Cardiac MRI
Quantifies MR severity by regurgitant volume and fraction. Assesses LV volumes and myocardial fibrosis. Useful when echo is inconclusive.
Right Heart Catheterisation
Measures pulmonary artery pressure, wedge pressure, and cardiac output. Confirms haemodynamic severity when non-invasive data are discordant.
What Happens If Left Untreated?
Progressive volume or pressure overload leads to irreversible cardiac damage.
LV Dilatation & Dysfunction (MR)
Chronic volume overload causes progressive LV enlargement and declining EF. Once LVESD exceeds 40 mm, post-operative LV dysfunction risk increases.
Pulmonary Hypertension (MS & MR)
Backward transmission of elevated LA pressure causes pulmonary hypertension, right ventricular dysfunction, and tricuspid regurgitation.
Atrial Fibrillation
LA enlargement from both MR and MS strongly predisposes to AF. AF worsens symptoms and introduces stroke risk requiring anticoagulation.
Thromboembolism (MS)
Stagnant blood in the enlarged LA in MS, especially with AF, forms clots that can cause stroke. Anticoagulation is essential in MS + AF.
Treatment Options for Mitral Valve Disease
Treatment depends on lesion type, severity, symptoms, and anatomy.
Mitral Valve Repair Surgery
Class I for severe symptomatic MRPreferred for primary degenerative MR. Valve-preserving surgery (leaflet resection, chordal repair, annuloplasty ring) avoids prosthesis-related complications.
MitraClip
COAPT: −47% HF hosp, −38% mortalityCatheter-based repair for secondary MR in HF patients. COAPT trial: −47% HF hospitalisation, −38% mortality. Requires strict patient selection.
Balloon Mitral Valvotomy (PBMV)
Preferred for suitable MS anatomyCatheter procedure for MS with suitable anatomy (Wilkins ≤8). Balloon splits fused rheumatic leaflets, doubling valve area.
Mitral Valve Replacement
When repair is not feasible. Mechanical valve (lifelong warfarin) or bioprosthetic valve (limited durability, no anticoagulation).
Medications for Mitral Valve Disease
Medical therapy focuses on symptom control and complication prevention.
Lifestyle Changes & Self-Care for Mitral Valve Disease
Healthy habits help manage symptoms and prevent complications.
Regular Echo Surveillance
Essential monitoringAnnual or bi-annual echo to monitor severity progression. Report any new or worsening symptoms immediately.
Salt Restriction
Reduces congestionLimit sodium to <2g/day to reduce fluid overload, especially if there is any HF component from MR or MS.
Moderate Exercise
As toleratedRegular gentle exercise as tolerated. Avoid heavy lifting and competitive sports in severe disease. Cardiac rehabilitation beneficial.
Infection Prevention
Endocarditis preventionGood dental hygiene and prompt treatment of infections. Antibiotic prophylaxis for dental procedures only if prosthetic valve or prior endocarditis.
Weight Management
Reduces haemodynamic burdenMaintain healthy BMI. Obesity increases LA pressure and worsens MR severity through volume overload.
Avoid Alcohol Excess
Reduces AF riskAlcohol can worsen AF and contribute to cardiomyopathy. Limit to 1–2 units per day.
Guidelines & Latest Evidence
Landmark trials define the contemporary management of mitral valve disease.
When to See a Doctor
Certain symptoms in mitral valve disease require prompt medical attention.
Worsening Breathlessness
Increasing dyspnoea, orthopnoea, or PND indicates disease progression or decompensation requiring echocardiographic re-evaluation.
New-Onset Atrial Fibrillation
Palpitations with irregular pulse in MVD requires ECG, echo, and anticoagulation assessment to prevent stroke.
Signs of Infection / Endocarditis
Fever, chills, night sweats, or new murmur requires blood cultures and echo to rule out infective endocarditis.
Chest Pain or Haemoptysis
Coughing blood in MS suggests pulmonary hypertension or pulmonary infarction. Chest pain may indicate endocarditis with embolisation.
Frequently Asked Questions
Guideline-directed explanations regarding mitral valve leaks and rheumatic stenoses.
Mitral regurgitation (MR) is a leaking mitral valve — blood flows backward from the left ventricle into the left atrium during systole instead of all going forward into the aorta. Primary MR is caused by structural valve abnormality (MVP, chordal rupture). Secondary functional MR occurs when a dilated, failing ventricle distorts a structurally normal valve. Severe primary MR requires surgery (repair preferred). Severe secondary MR in heart failure may benefit from MitraClip (COAPT: −47% HF hospitalisation, −38% mortality) after optimising heart failure medications.
Mitral stenosis is narrowing of the mitral valve, obstructing blood flow from left atrium to left ventricle. In India, the dominant cause is rheumatic heart disease — valve damage following childhood streptococcal throat infection and rheumatic fever. Severe MS (MVA <1.0 cm²) causes breathlessness, atrial fibrillation, pulmonary hypertension, and haemoptysis. The preferred treatment for suitable anatomy is balloon mitral valvotomy (PBMV) — a catheter procedure that separates fused valve leaflets without open-chest surgery.
MitraClip is a catheter-based mitral valve repair procedure that clips the mitral leaflets together to reduce regurgitation — without open-chest surgery. It is approved for secondary MR in heart failure patients who remain symptomatic despite optimal medical therapy. COAPT (NEJM 2018) showed MitraClip reduced HF hospitalisation by 47% and mortality by 38% versus medical therapy in carefully selected patients.
Surgery is indicated for severe primary mitral regurgitation if you have any symptoms (breathlessness, fatigue, palpitations), or if your ejection fraction has dropped below 60%, or if the left ventricle has dilated beyond 40 mm in end-systolic diameter — even without symptoms. For mitral stenosis, intervention is needed when the valve area is severely narrowed (<1.0 cm²) or if you develop symptoms, atrial fibrillation, or pulmonary hypertension. Whenever possible, mitral valve repair is preferred over replacement as it preserves the native valve structure and avoids long-term anticoagulation. The exact timing and type of intervention are determined by echocardiographic measurements and your individual clinical profile.
Mild mitral regurgitation (MR) discovered incidentally on echocardiography often remains stable for years and may even improve with treatment of the underlying cause. In secondary (functional) MR caused by heart failure, optimising GDMT — particularly ARNi, beta-blockers, and SGLT2 inhibitors — can reduce the severity of MR by improving ventricular function and reducing mitral annular dilation. However, moderate-to-severe primary MR (caused by structural valve disease such as flail leaflet or chordal rupture) does not heal on its own and will typically progress over time. Surgery or transcatheter intervention is indicated when the regurgitation becomes severe or causes symptoms, LV dilation, or declining EF.
Mitral valve prolapse (MVP) is a condition where the mitral valve leaflets bulge (prolapse) back into the left atrium during the heart's contraction. It is relatively common, affecting 2–3% of the population. Most people with MVP have no symptoms and require no treatment other than periodic echocardiographic follow-up. However, some patients with MVP develop significant mitral regurgitation that may eventually require surgery. A small subset of patients with MVP — particularly those with 'arrythmogenic MVP' — may be at risk for ventricular arrhythmias. MVP is usually diagnosed on echocardiography, and follow-up is guided by the severity of associated MR and any symptoms.
The frequency of echocardiographic follow-up depends on the severity of the valve disease. For mild MR or MS with no symptoms, echocardiography every 2–3 years is sufficient. For moderate disease, annual or biannual echo is recommended. For severe MR without symptoms, echocardiography should be performed every 6–12 months to monitor LV function and dimensions — as surgery is indicated when EF drops below 60% or LVESD exceeds 40 mm. For severe MS, echo every 6–12 months monitors valve area and pulmonary pressures. After valve repair or replacement, a baseline post-procedure echo is performed and then annually or biennially depending on valve type and clinical status.
Pregnancy with mitral valve disease requires careful pre-conception counselling and multidisciplinary management by a cardiologist and obstetrician. Women with mild MR or MS and normal cardiac function usually tolerate pregnancy well with close monitoring. However, moderate-to-severe MS is poorly tolerated during pregnancy — the increased blood volume and heart rate of pregnancy can cause rapid decompensation with pulmonary oedema. Ideally, significant valve disease should be treated before pregnancy (with PBMV for MS or surgery for MR). Women with mechanical prosthetic valves face particular challenges due to the need for anticoagulation (warfarin is teratogenic; heparin requires careful management). All pregnant women with mitral valve disease should be managed in a specialist cardio-obstetric clinic.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.

MitraClip Repair
Catheter-based mitral valve repair for secondary MR in heart failure.

2D Echocardiography
Comprehensive Doppler grading of MR severity and Wilkins score for MS.
Aortic Stenosis
Coexisting valve disease evaluation and surgical planning.

Heart Failure
Secondary MR management in the context of heart failure therapy.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.