
Shortness of Breath
Shortness of breath (dyspnoea) is a critical presenting symptom in cardiology. While respiratory causes are common, breathlessness can be the sole indicator of silent ischaemia or progressive heart failure.
Cardiac Causes of Exertional Breathlessness
When cardiac efficiency drops, fluid backup or supply-demand mismatch creates severe dyspnoea.
Shortness of breath on exertion is one of the most common cardiac symptoms. It can result from heart failure (fluid backup into the lungs), coronary artery disease (ischaemia causing diastolic dysfunction), or valvular disease. In diabetics and the elderly, breathlessness may be the only warning sign of heart disease.
Cardiac & Non-Cardiac Causes of Breathlessness
Breathlessness can arise from cardiac, respiratory, haematological, or psychological causes.
Heart Failure (HFrEF / HFpEF)
The most common cardiac cause. The heart cannot pump efficiently, causing fluid to back up into the lungs (pulmonary congestion) and reducing oxygen delivery to the body.
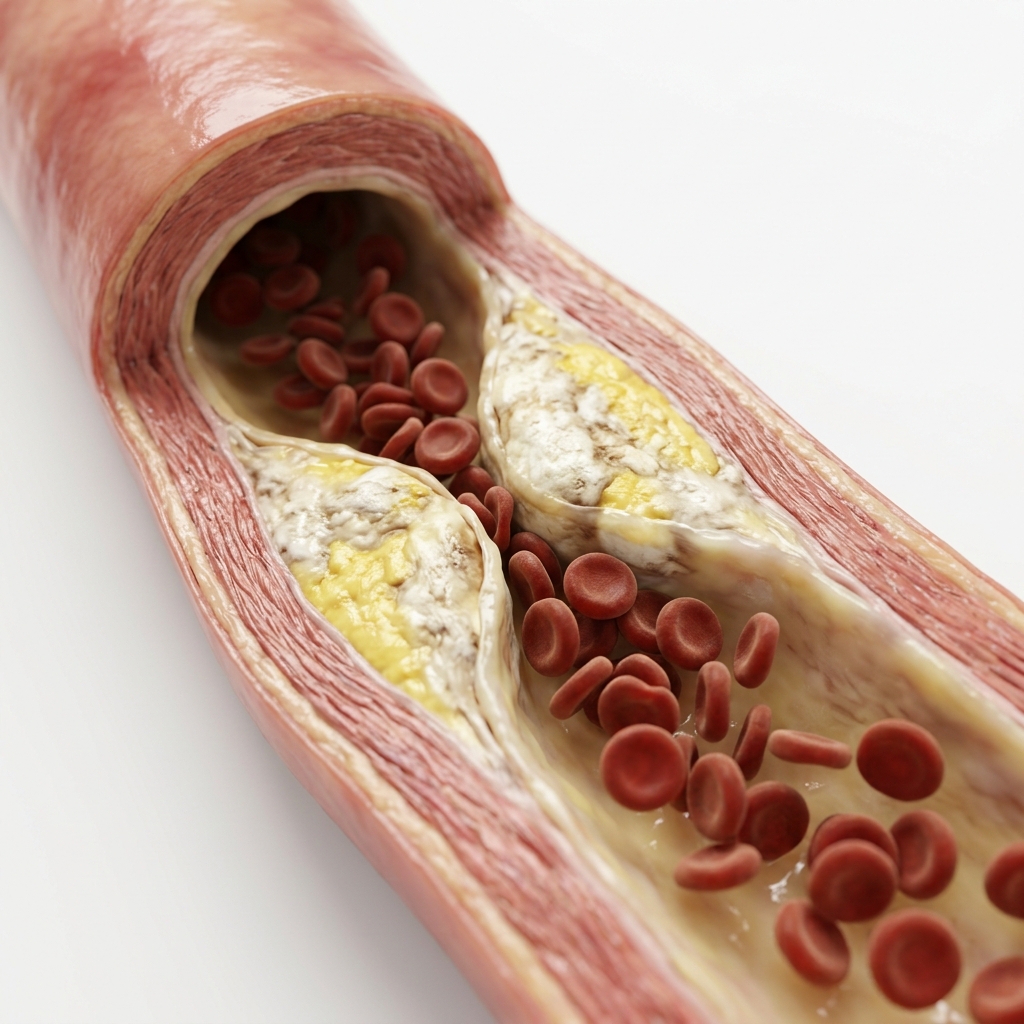
Coronary Artery Disease (CAD)
Breathlessness can be the only warning sign of significant CAD — particularly in diabetics, women, and the elderly who often have silent ischaemia without classic chest pain.
Valvular Disease & Arrhythmias
Aortic stenosis, mitral regurgitation, atrial fibrillation with rapid ventricular rate, VT, and heart block can all present primarily with breathlessness.
Respiratory Disease
Asthma, COPD, and interstitial lung disease. Typically associated with cough, wheeze, and smoking history. Pulmonary function tests differentiate obstructive from restrictive patterns.
Pulmonary Embolism
Sudden-onset breathlessness with sharp pleuritic chest pain. Risk factors include surgery, immobility, long-haul travel, and malignancy.
Anaemia & Anxiety
Reduced haemoglobin lowers oxygen-carrying capacity. Anxiety and panic disorder can closely mimic acute coronary syndrome — always complete cardiac exclusion first.
Types & Severity of Breathlessness
Dyspnoea is classified by onset, severity, and underlying mechanism.
Signs & Symptoms Associated with Breathlessness
Associated symptoms help determine the underlying cause of dyspnoea.
Orthopnoea & PND
Breathlessness when lying flat, relieved by sitting up (orthopnoea). Waking suddenly gasping for air (PND) is classic for heart failure — indicates significantly elevated LV filling pressures.
Bilateral Ankle Swelling
Right-sided backlog causes dependent fluid build-up. Progressive dyspnoea with bilateral ankle oedema, fatigue, and reduced exercise tolerance indicates worsening heart failure.
Cough & Wheeze
Productive cough with sputum, wheezing, and smoking history suggests respiratory cause. Cardiac asthma mimics bronchial asthma — BNP helps differentiate.
Chest Pain or Pressure
Combined chest pain and dyspnoea is a high-risk presentation for acute coronary syndrome or pulmonary embolism.
How We Investigate Shortness of Breath
We apply rapid biomarker assessment and ultrasound imaging within a single clinical visit.
Resting 12-Lead ECG
First-line test — detects ischaemia, arrhythmia, LV hypertrophy, and prior myocardial infarction. Performed in 5 minutes with immediate result.
BNP / NT-proBNP
Biomarker for heart failure. Elevated BNP distinguishes cardiac from non-cardiac causes of breathlessness with high sensitivity and specificity.
2D Echocardiography
Assesses LV function, wall motion, pulmonary pressures, and valve disease — the key test for cardiac dyspnoea. Identifies HFrEF, HFpEF, and pulmonary hypertension.
Chest X-Ray
Detects cardiomegaly, pulmonary congestion, and respiratory causes like pneumonia, pneumothorax, or COPD changes.
Treadmill Stress Test / CT Coronary Angio
Detects exercise-induced ischaemia. CT coronary angiography for non-invasive coronary anatomy if CAD is suspected.
What Happens If Left Untreated?
Ignoring cardiac breathlessness can lead to progressive heart failure and adverse outcomes.
Progressive Heart Failure
Untreated HF causes worsening pulmonary congestion, reduced exercise capacity, and frequent hospitalisations. NYHA class worsens over time.
Silent MI Progression
In diabetics, breathlessness may be the only sign of ACS. Delayed treatment leads to larger infarcts and worse LV function.
Respiratory Complications
Chronic pulmonary congestion from untreated HF leads to pleural effusions, pulmonary fibrosis, and respiratory failure.
Reduced Quality of Life
Persistent dyspnoea limits daily activities, reduces independence, and is associated with depression and social isolation.
Treatment Options for Cardiac Breathlessness
Treatment targets the underlying cause of dyspnoea.
Heart Failure Therapy (GDMT)
Diuretics for congestion, ACEi/ARNi, beta-blockers, MRA, and SGLT2i for HFrEF. SGLT2i for HFpEF. Four-pillar therapy reduces mortality by >50%.
CAD Revascularisation
PCI or CABG for significant coronary blockages. Relieves ischaemia-mediated diastolic dysfunction and improves exercise tolerance.
Valve Intervention
TAVR for aortic stenosis, MitraClip for mitral regurgitation, PBMV for mitral stenosis. Valve correction dramatically improves symptoms.
Treat Non-Cardiac Causes
Bronchodilators for COPD, anticoagulation for PE, iron supplementation for anaemia, and CBT for anxiety.
Medications for Cardiac Breathlessness
Drug therapy is directed at the underlying cardiac condition causing dyspnoea.
Lifestyle Changes & Self-Care for Breathlessness
Daily self-management strategies can improve symptoms and prevent deterioration.
Sleep Upright or Propped Up
Reduces nocturnal dyspnoeaSleep with 2–3 pillows or in a recliner to reduce orthopnoea. Elevating the head decreases pulmonary congestion.
Paced Activity & Rehabilitation
Improves functional capacityCardiac or pulmonary rehabilitation improves exercise tolerance. Learn to pace activities and take rest breaks.
Daily Weight Monitoring
Early detection of congestionWeigh every morning. Gain >2 kg in 3 days = fluid overload. Contact your doctor for diuretic adjustment.
Salt & Fluid Management
Reduces fluid overloadLimit sodium to <2g/day. Fluid restriction (1.5–2 L/day) in advanced HF with hyponatraemia.
Smoking Cessation
Essential for all causesSmoking worsens both cardiac and respiratory causes of breathlessness. Quitting improves symptoms and reduces disease progression.
Pursed-Lip Breathing
Self-management techniqueBreathe in through nose, out through pursed lips (like blowing out a candle). This technique reduces air trapping and dyspnoea.
Guidelines & Latest Evidence
Current guidelines inform the evaluation of dyspnoea and management of underlying causes.
Red Flag Markers: Immediate Action Required
Watch for critical emergency signs that indicate acute decompensated heart failure or massive emboli.
Sudden or Severe Breathlessness at Rest
May indicate acute pulmonary oedema, massive pulmonary embolism, or acute coronary syndrome — requires immediate emergency evaluation.
Breathlessness with Chest Pain or Pressure
Combined chest pain and dyspnoea is a high-risk presentation for acute coronary syndrome or pulmonary embolism.
Waking Up Gasping for Air (PND)
Paroxysmal nocturnal dyspnoea is classic for heart failure — indicates significantly elevated left ventricular filling pressures.
Breathlessness in a Diabetic Patient
Diabetics often have silent ischaemia. Any new breathlessness or exercise intolerance in a diabetic should be treated as cardiac until proven otherwise.
Breathlessness with Leg Swelling
Progressive dyspnoea with bilateral ankle oedema, fatigue, and reduced exercise tolerance indicates worsening heart failure.
Breathlessness After Surgery or Long Travel
Sudden onset dyspnoea following surgery, prolonged immobility, or long-haul flights strongly suggests pulmonary embolism.
Frequently Asked Questions
Guideline-directed clarifications regarding structural fluid backup and silent ischaemia.
Yes — particularly in diabetics, women, and the elderly. Cardiac ischaemia often presents atypically: breathlessness or epigastric discomfort alone, without classic chest pain. Diabetics have autonomic neuropathy that reduces anginal perception, so any new breathlessness or exercise intolerance in a diabetic should be treated as possible cardiac ischaemia until proven otherwise. Heart failure also commonly presents with progressive exertional dyspnoea, orthopnoea (breathlessness lying flat), and paroxysmal nocturnal dyspnoea — waking up gasping for air at night.
Cardiac dyspnoea is typically exertional, progressive over weeks to months, associated with orthopnoea (worse lying flat), PND (waking up gasping), and leg swelling. Respiratory dyspnoea is more commonly associated with cough, wheeze, sputum production, and a prior smoking history. However, the overlap is substantial — heart failure and COPD frequently coexist. Formal testing including ECG, echo, BNP, and pulmonary function tests is the only reliable way to distinguish cardiac from respiratory causes.
Initial evaluation: resting 12-lead ECG (detects ischaemia, arrhythmia, LVH), high-sensitivity troponin (rules out NSTEMI), chest X-ray (cardiomegaly, pulmonary congestion), 2D echocardiography (LV function, wall motion, valve disease, pulmonary pressures), and BNP or NT-proBNP (heart failure marker). If these are normal, pulmonary function tests (asthma, COPD), D-dimer (pulmonary embolism), and full blood count (anaemia) help identify non-cardiac causes. Stress testing or CT coronary angiography may be indicated if CAD is suspected.
You should see a cardiologist if you experience: progressive breathlessness on exertion that has worsened over weeks to months; orthopnoea (needing extra pillows to sleep); waking up gasping for air; breathlessness with chest discomfort or palpitations; or any new breathlessness if you have diabetes, hypertension, or a family history of heart disease. Unexplained breathlessness in anyone over 40 with risk factors warrants cardiac evaluation. Do not wait — early diagnosis of heart failure or CAD dramatically improves outcomes.
Cardiac breathlessness (dyspnoea from heart disease) typically worsens with exertion and is associated with orthopnoea — difficulty breathing when lying flat, requiring extra pillows at night. Patients often wake up suddenly gasping for air (paroxysmal nocturnal dyspnoea) and may have ankle swelling. Respiratory breathlessness is more often associated with cough, wheeze, sputum production, and a history of smoking or asthma. However, the symptoms overlap substantially — many patients have both cardiac and respiratory disease (cardiometabolic syndrome). Formal testing with ECG, echocardiography, BNP blood test, chest X-ray, and pulmonary function tests is the only reliable way to distinguish cardiac from respiratory causes.
Yes — anaemia is a common and under-recognised cause of breathlessness. Haemoglobin carries oxygen from the lungs to the tissues. When haemoglobin levels drop, the body compensates by increasing heart rate and breathing rate — leading to the sensation of breathlessness, especially on exertion. Severe anaemia (haemoglobin below 8 g/dL) can closely mimic heart failure, causing fatigue, pallor, breathlessness, and even elevated heart rate. A complete blood count is a simple test that should be part of the initial evaluation for any patient presenting with unexplained dyspnoea. Treating the underlying cause of anaemia (iron deficiency, vitamin B12 deficiency, chronic disease) often significantly improves symptoms.
Paroxysmal nocturnal dyspnoea (PND) is a classic symptom of heart failure. The patient goes to bed breathing comfortably but wakes up 1–3 hours later suddenly gasping for air, with a feeling of suffocation. This occurs because lying flat causes fluid from the legs and abdomen to redistribute into the central circulation. A failing heart cannot handle this increased volume, causing fluid to accumulate in the lungs (pulmonary congestion). Patients typically sit up, dangle their legs, or go to a window for fresh air, and symptoms gradually resolve over 15–30 minutes. PND is distinct from simple orthopnoea (breathlessness on lying flat) — it is a more severe indicator of elevated left ventricular filling pressures and warrants urgent medical evaluation.
Emergency evaluation of acute shortness of breath follows a structured pathway. The first step is clinical assessment including vital signs, oxygen saturation, lung auscultation, and examination for signs of heart failure (elevated JVP, leg oedema). Immediate tests include: 12-lead ECG (to detect ischaemia, arrhythmia, or LVH), chest X-ray (cardiomegaly, pulmonary congestion, pneumonia), and high-sensitivity troponin (to rule out heart attack). BNP or NT-proBNP blood test is the key biomarker to distinguish cardiac from respiratory causes — a normal BNP effectively rules out heart failure. If pulmonary embolism is suspected, D-dimer and CT pulmonary angiography are performed. This systematic approach allows rapid identification of life-threatening causes.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.

2D Echocardiography
Key test for cardiac dyspnoea — EF, pulmonary pressures, and valve disease.

Resting ECG
First-line test detecting ischaemia, arrhythmia, LVH, and prior MI.
Heart Failure
The most common cardiac cause of breathlessness — full diagnostic workup.
Coronary Artery Disease
Silent ischaemia presenting as breathlessness — especially in diabetics.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.