
Diabetic Heart Disease
Cardiovascular disease causes 50–80% of deaths in people with type 2 diabetes. Hyperglycaemia accelerates plaque build-up, blocks small blood vessels, and blunts anginal pain perception — leading to silent heart attacks.
Diabetes & Cardiovascular Risk Stratification
Diabetes doubles the risk of heart attack in men and triples it in women — requiring precise screening.
Elevated blood glucose damages the delicate vascular endothelium and drives aggressive plaque deposits. Unrecognized heart attacks represent a primary threat due to blunted neural pathways.
Five Pathways of Diabetic Vascular Damage
Understanding the cellular and mechanical processes driving accelerated coronary stenosis in diabetes.
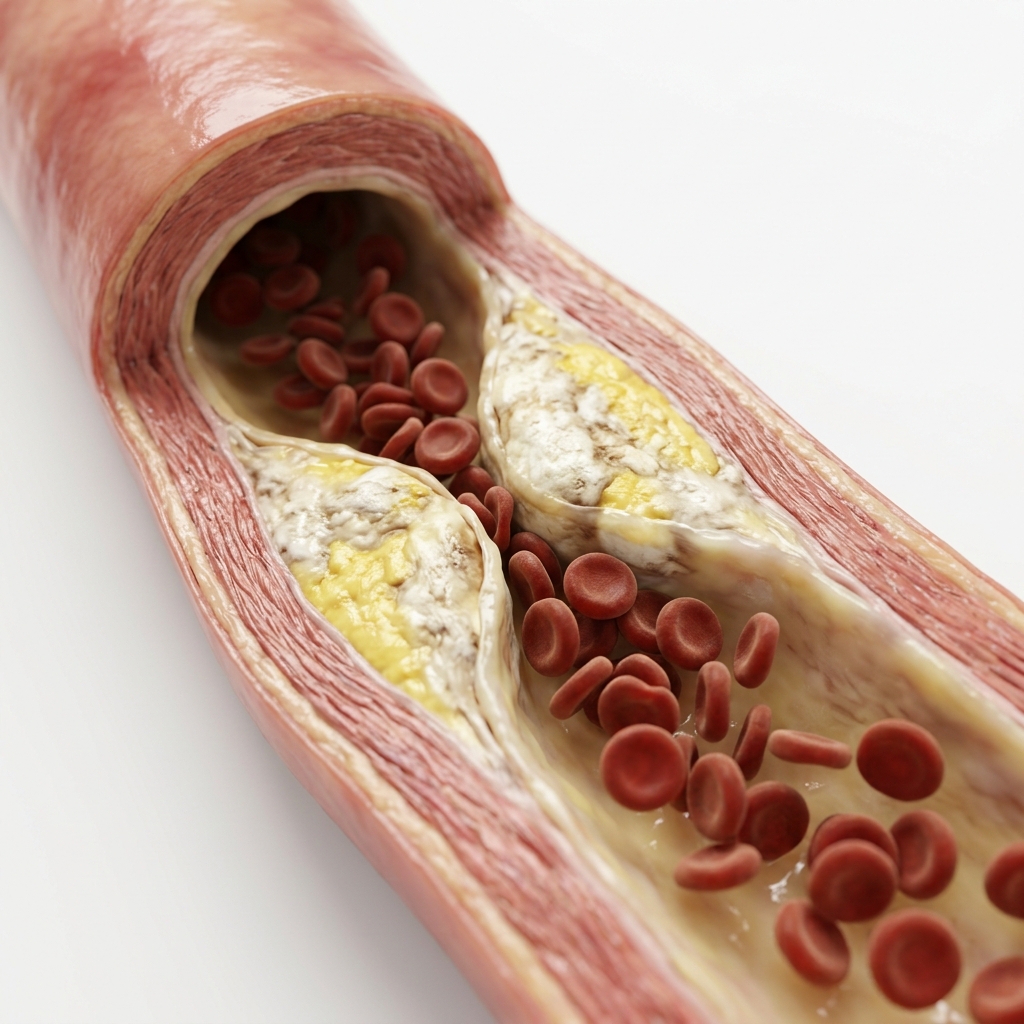
Accelerated Atherosclerosis
Hyperglycaemia damages the endothelium and drives inflammatory plaque formation. Diabetics develop coronary disease 7–10 years earlier and in more vessels than non-diabetics.
Diabetic Cardiomyopathy
Hyperglycaemia directly damages heart muscle fibres independently of coronary disease — causing diastolic dysfunction, LV stiffness, and eventually HFpEF even in the absence of any coronary blockages.
Silent Ischaemia
Autonomic neuropathy reduces or abolishes anginal pain perception. Approximately 25–35% of diabetics with significant coronary disease experience no chest pain. ECG and echo screening is therefore essential.
Diabetic Kidney Disease
CKD in diabetes markedly amplifies cardiovascular risk. eGFR <60 mL/min or significant albuminuria classifies the patient as Very High CV risk — LDL target <1.4 mmol/L required.
Atrial Fibrillation Risk
Type 2 diabetes increases AF risk by approximately 40%. AF in diabetics carries higher stroke risk — both the diabetes and the AF independently elevate CHA₂DS₂-VASc score.
Types & Severity of Diabetic Heart Disease
Diabetic heart disease exists on a spectrum from subclinical dysfunction to advanced multi-vessel disease.
Signs & Symptoms of Diabetic Heart Disease
Symptoms may be atypical or absent due to autonomic neuropathy.
Silent Ischaemia
Autonomic neuropathy damages the nerve fibres that would normally transmit chest pain — so many diabetics have extensive coronary artery disease or even suffer heart attacks without any warning.
Breathlessness on Exertion
Any breathlessness or reduced exercise tolerance in a diabetic should trigger cardiac investigation — treat it as angina until proven otherwise.
Atypical Chest Discomfort
When chest pain does occur, it may present as epigastric discomfort, indigestion, or vague pressure rather than classic angina.
Fatigue & Reduced Capacity
Unexplained fatigue or decline in exercise capacity may be the only manifestation of underlying coronary disease or diabetic cardiomyopathy.
How Is Diabetic Heart Disease Diagnosed?
Annual structured screening is essential to detect silent ischaemia and monitor cardiac function.
Resting ECG
Detects silent ischaemia (Q waves from unrecognised MI), LVH from hypertension, conduction abnormalities, and baseline arrhythmias. Annual screening recommended.
2D Echocardiography
Detects LV hypertrophy, diastolic dysfunction (early HFpEF), EF, and valve disease. Baseline echo recommended in all diabetics with hypertension. Repeat every 2–3 years.
Treadmill Stress Test
Any breathlessness, reduced exercise tolerance, or exertional fatigue in a diabetic should trigger a TMT or CT coronary angiography to exclude ischaemia.
Lipid Profile & Renal Function
LDL target <1.4 mmol/L in very high-risk diabetics. eGFR + urine albumin:creatinine ratio monitors kidney disease and amplifies CV risk stratification.
Comprehensive Risk Assessment
Full SCORE2 calculation, medication review, SGLT2 inhibitor optimisation, and personalised prevention plan coordinated between cardiologist and diabetologist.
What Happens If Left Untreated?
Uncontrolled diabetic heart disease leads to progressive cardiac damage and increased mortality.
Progressive LV Dysfunction
Untreated diabetic cardiomyopathy progresses from diastolic dysfunction to systolic failure, with declining EF and worsening symptoms.
Higher Stroke Risk
Diabetes independently increases stroke risk. Combined with AF, the risk multiplies significantly.
Silent Heart Attack
A first presentation may be a silent MI — unrecognised until ECG shows Q waves. Delayed treatment worsens outcomes.
Accelerated Kidney Disease
Diabetic nephropathy progresses faster with uncontrolled cardiovascular risk, leading to dialysis dependence.
SGLT2 Inhibitors: Empagliflozin & Dapagliflozin
Standard-of-care medications that reduce cardiovascular risk and heart failure hospitalization, independent of glucose-lowering.
Empagliflozin
EMPA-REG OUTCOME (NEJM 2015)EMPA-REG OUTCOME showed a 38% reduction in cardiovascular death and a 35% drop in heart failure hospitalizations in type 2 diabetes patients with established heart disease.
Dapagliflozin
DAPA-HF (NEJM 2019)DAPA-HF demonstrated a 26% reduction in worsening HF or CV death in HFrEF — including patients without diabetes.
GLP-1 Receptor Agonists
LEADER / SUSTAIN-6Semaglutide and liraglutide reduce MACE in diabetes. LEADER: liraglutide −13% MACE. SUSTAIN-6: semaglutide −26% MACE.
Comprehensive Risk Management
ESC 2023 GuidelinesLDL target <1.4 mmol/L (≥50% reduction), BP target <130/80 mmHg, HbA1c target <7.0%. Aspirin for secondary prevention only.
Cardiovascular Targets & Treatment Targets
We enforce rigorous cardiometabolic targets across multiple parameters to minimize absolute clinical risk.
Lifestyle Changes & Self-Care for Diabetic Heart Disease
Lifestyle modifications are the foundation of cardiometabolic risk reduction.
Regular Exercise
Improves HbA1c by 0.5–1.0%150 minutes per week of moderate aerobic activity. Exercise improves insulin sensitivity, lowers BP, and reduces cardiovascular events.
Heart-Healthy Diet
Reduces MACE by 25–30%Mediterranean or DASH diet rich in fruits, vegetables, whole grains, and lean protein. Low in saturated fat and refined carbohydrates.
Weight Management
5–10% weight loss: −0.5–1.0% HbA1cTarget BMI <25 kg/m². Weight loss of 5–10% improves glycaemic control, lipids, and BP. Bariatric surgery considered if BMI >35.
Glucose Monitoring
Target HbA1c <7.0%Regular self-monitoring of blood glucose and quarterly HbA1c checks. Continuous glucose monitoring (CGM) for patients on insulin.
Smoking Cessation
−50% CV risk within 1 yearSmoking dramatically amplifies cardiovascular risk in diabetes. Risk of MI halves within 1 year of quitting.
Limit Alcohol
Maximum 14 units/weekAlcohol can cause hypoglycaemia and raises BP. Limit to 1–2 units per day. Avoid binge drinking.
Guidelines & Latest Evidence
Major trials guide the management of diabetic heart disease.
When to See a Doctor
Prompt evaluation is critical given the high prevalence of silent ischaemia in diabetes.
New or Worsening Breathlessness
Any breathlessness or reduced exercise tolerance in a diabetic should be treated as cardiac until proven otherwise — it may be the only sign of ischaemia or heart failure.
Chest Discomfort or Epigastric Pain
Atypical presentations are common in diabetes. Indigestion, nausea, or vague upper abdominal pain may be angina or MI.
Rapid Weight Gain or Leg Swelling
Sudden weight gain (>2 kg in 3 days) or bilateral ankle oedema may indicate heart failure decompensation.
Poorly Controlled Risk Factors
Persistent HbA1c >8.0%, BP above target, or LDL above target despite medication warrants specialist review.
Frequently Asked Questions
Guideline-directed clarifications regarding metabolic blockages and silent heart attacks.
Diabetes increases heart disease risk through direct endothelial injury from hyperglycaemia (accelerating atherosclerosis), small vessel disease (microangiopathy) affecting the coronary microcirculation, diabetic cardiomyopathy (direct heart muscle damage), autonomic neuropathy (causes silent ischaemia — heart attacks without chest pain), and kidney disease (which further amplifies cardiovascular risk). Cardiovascular disease causes 50–80% of deaths in people with type 2 diabetes. All diabetics require structured annual cardiac assessment and aggressive risk factor management.
Silent ischaemia is reduced blood flow to the heart without any chest pain symptoms. In diabetics, autonomic neuropathy damages the nerve fibres that would normally transmit chest pain — so many diabetics have extensive coronary artery disease or even suffer heart attacks without any warning. Annual ECG and echocardiography can detect evidence of silent ischaemia (Q waves from unrecognised MI, wall motion abnormalities). Any breathlessness or reduced exercise tolerance in a diabetic should trigger cardiac investigation — treat it as angina until proven otherwise.
SGLT2 inhibitors (empagliflozin, dapagliflozin) lower blood glucose but were found to dramatically reduce cardiovascular mortality and heart failure — independent of glucose lowering. EMPA-REG OUTCOME showed empagliflozin reduced cardiovascular death by 38% and HF hospitalisation by 35% in diabetics with established CV disease. DAPA-HF showed dapagliflozin reduced worsening HF or CV death by 26% in HFrEF — including patients without diabetes. They are recommended for all diabetics with established CVD or high CV risk, and for all HFrEF patients regardless of diabetes status.
For multi-vessel coronary disease in diabetics, bypass surgery (CABG) is preferred over angioplasty (PCI). The FREEDOM trial (NEJM 2012, n=1,900) showed CABG reduced the 5-year composite of death, MI, and stroke by 26% versus PCI in diabetics with multi-vessel disease. Current ESC and AHA guidelines recommend CABG for diabetics with significant multi-vessel CAD. CABG achieves more complete revascularisation of the diffuse, small-vessel disease typical in diabetics. Single-vessel disease and low-complexity anatomy remain appropriate for PCI.
The general HbA1c target for most adults with type 2 diabetes is below 7.0% (53 mmol/mol). However, for patients with established cardiovascular disease, the target is individualised — stricter control (<6.5%) may benefit younger patients with recent-onset diabetes, while less strict targets (<8.0%) are appropriate for elderly patients, those with long-standing diabetes, or those with a history of severe hypoglycaemia. The ACCORD trial found that intensive glucose lowering increased mortality in high-risk patients with long-standing diabetes, so aggressive targets are not recommended for this group. All HbA1c targets should be achieved without causing significant hypoglycaemia.
Yes — most patients with diabetes and any additional risk factor (age >40, hypertension, smoking, family history of heart disease, or evidence of kidney disease) should be on a moderate-to-high intensity statin regardless of their baseline LDL cholesterol level. Diabetes itself is a powerful risk enhancer, placing most diabetic patients in the high or very high cardiovascular risk category. The target LDL cholesterol for very high-risk diabetics is below 1.4 mmol/L (55 mg/dL), and a ≥50% reduction from baseline. Statin therapy reduces major cardiovascular events by approximately 25% in diabetics, with benefits extending to those who have never had a heart attack.
Regular aerobic exercise can significantly improve cardiac function in diabetics with heart disease. Exercise improves insulin sensitivity, reduces HbA1c, lowers blood pressure, improves lipid profiles, and enhances endothelial function — all of which reduce the metabolic stress on the heart. In diabetic cardiomyopathy, structured exercise training has been shown to improve diastolic function, reduce LV stiffness, and increase exercise capacity. The ESC recommends at least 150 minutes per week of moderate-intensity aerobic activity (brisk walking, cycling, swimming) for all diabetic patients. Resistance training twice weekly provides additional metabolic benefits. Always obtain cardiac clearance before starting a new exercise programme.
All patients with type 2 diabetes should have a baseline cardiac assessment at the time of diagnosis, including ECG, blood pressure measurement, and lipid profile. If the baseline evaluation is normal, annual cardiac review is recommended — including ECG, echocardiography every 2–3 years, and cardiac risk scoring. Diabetics with established cardiovascular disease or with additional risk factors (hypertension, smoking, family history, or abnormal ECG) should be seen every 6–12 months. Any new symptom — particularly breathlessness, reduced exercise tolerance, palpitations, or atypical chest discomfort — warrants immediate cardiology evaluation, as diabetics frequently have silent ischaemia without chest pain.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.

Cardiac Risk Assessment
Comprehensive SCORE2 risk profiling for diabetics with metabolic syndrome.
Coronary Artery Disease
Silent ischaemia detection and comprehensive CAD management in diabetics.

Treadmill Stress Test
Exercise ECG to detect silent ischaemia in diabetic patients.

Heart Failure
Diabetic cardiomyopathy and HFpEF evaluation and management.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.