
Understanding Chest Pain
Chest pain is one of the most common presentations in cardiology — and one of the most important to evaluate correctly. Learn to distinguish cardiac from non-cardiac causes.
What Does Cardiac Chest Pain Feel Like?
Typical cardiac discomfort is described as crushing central pressure or tightness provoked by physical effort.
Cardiac chest pain from coronary blockages (angina or heart attack) usually manifests as central or left-sided tightness, squeezing, or heaviness, radiating to the neck, jaw, back, or left arm.
Causes & Risk Factors for Chest Pain
Chest pain can arise from cardiac, vascular, respiratory, gastrointestinal, or musculoskeletal causes.
Coronary Artery Disease
Atherosclerotic plaque narrowing the coronary arteries. Angina occurs when myocardial oxygen demand exceeds supply — typically during exertion or emotional stress.
Acute Coronary Syndrome
Plaque rupture with thrombus formation causes unstable angina, NSTEMI, or STEMI. This is a medical emergency requiring immediate catheterisation.
Aortic Stenosis
Severe aortic valve narrowing causes exertional chest pain (angina) due to pressure overload and reduced cardiac output. Part of the classic symptom triad.
Aortic Dissection
Tearing chest pain radiating to the back. A surgical emergency. Hypertension is the most important risk factor.
Pulmonary Causes
Pulmonary embolism (sharp pain + breathlessness), pleurisy (pain on inspiration), pneumothorax (sudden unilateral pain).
Non-Cardiac Causes
Costochondritis (reproducible on palpation), GERD (burning, worse after meals), anxiety/panic attacks, and oesophageal spasm can all mimic cardiac pain.
Types & Severity of Chest Pain
Chest pain is classified by its underlying cause and urgency of treatment.
Signs & Symptoms
Cardiac chest pain patterns help distinguish ischaemia from other causes.
Typical Cardiac Pain
Central or left-sided squeezing, pressure, or heaviness. Radiates to the left arm, jaw, neck, or back. Provoked by physical exertion, cold air, or emotional stress.
Associated Symptoms
Sweating (diaphoresis) during chest pain is a strong objective indicator of significant myocardial ischaemia. Nausea, vomiting, and breathlessness are also common.
Atypical Presentations
Particularly in diabetic patients, women, and the elderly, ischaemia may present without chest pain. Shortness of breath, sudden fatigue, or epigastric discomfort are common.
Radiation Patterns
Pain may radiate to the left arm (ulnar aspect), neck, jaw, teeth, or back. Inferior MI often presents with epigastric pain, nausea, and vomiting.
Standardized Chest Pain Investigation Steps
We employ a structured, evidence-based cascade of tests to verify coronary perfusion.
Resting 12-Lead ECG
First investigation completed within minutes. Identifies STEMI needing emergency catheterization, prior MI scars, LBBB, or ischaemic T-wave inversions. A normal resting ECG does not rule out CAD.
High-Sensitivity Troponin Blood Profile
Cardio-specific biomarkers that rise within 1–3 hours of myocardial cellular injury. Essential for excluding acute NSTEMI or micro-infarcts.
Color Doppler 2D Echocardiography
Direct cardiac ultrasound scanning to evaluate regional wall motion abnormalities (RWMA), left ventricular EF, aortic valve narrowing, and pericardial fluid.
Treadmill Stress Test (TMT) / CT Coronary Angio
TMT assesses electrocardiographic changes under metabolic load. Non-invasive CT coronary angiography directly highlights calcification and luminal narrowing without catheter entry.
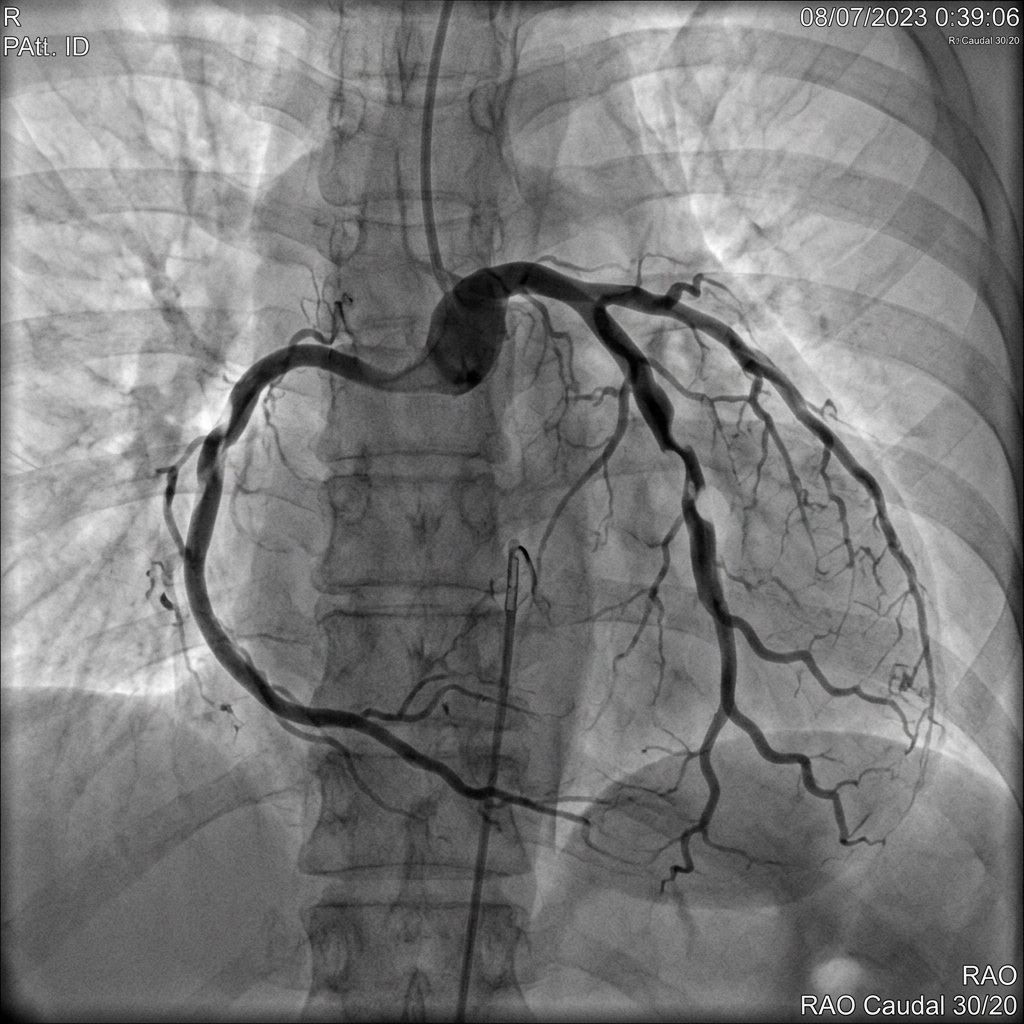
Invasive Coronary Angiography with FFR
The definitive diagnostic gold-standard. Catheter-directed dye injection highlights narrowing, and fractional flow reserve (FFR) determines if blockages require a stent.
What Happens If Left Untreated?
Ignoring cardiac chest pain can lead to irreversible heart muscle damage and death.
Myocardial Infarction
Unstable angina or untreated ischaemia can progress to complete coronary occlusion and heart attack. Every minute of delay causes more muscle death.
Heart Failure
Repeated or extensive infarction reduces left ventricular function, leading to heart failure, reduced exercise capacity, and poor prognosis.
Ventricular Arrhythmias & Sudden Death
Acute ischaemia can trigger ventricular tachycardia or fibrillation. Urgent defibrillation is required to prevent sudden cardiac death.
Progressive CAD
Atherosclerosis is a progressive disease. Without treatment, plaque burden increases, leading to more severe symptoms and higher risk of acute events.
Treatment Options for Chest Pain
Treatment depends on the underlying cause — from lifestyle modification to emergent revascularisation.
Medical Therapy for Angina
Antiplatelets (aspirin), statins (high-intensity), beta-blockers, and nitrates for symptom relief. Risk factor control including BP, lipids, and diabetes.
Percutaneous Coronary Intervention (PCI)
Angioplasty and stenting for significant coronary blockages. Radial artery access preferred for lower bleeding risk. IVUS/OCT guidance optimises results.
Coronary Artery Bypass Surgery (CABG)
For multi-vessel disease, left main disease, or diabetes with complex CAD. Bypass grafts restore blood flow around occluded segments.
Treat Underlying Non-Cardiac Cause
GERD treated with PPIs. Costochondritis with NSAIDs. Anxiety with cognitive behavioural therapy. Pulmonary embolism requires anticoagulation.
Medications for Cardiac Chest Pain
Drug therapy for ischaemic heart disease focuses on symptom relief, event prevention, and risk factor control.
Lifestyle Changes & Risk Factor Modification
Lifestyle interventions are the cornerstone of secondary prevention for coronary disease.
Smoking Cessation
−50% CV risk within 1 yearThe single most effective preventive measure. Risk of MI declines by 50% within 1 year of quitting.
Heart-Healthy Diet
Reduces MACE by 25–30%Mediterranean diet rich in fruits, vegetables, whole grains, olive oil, and fish. Low in saturated fat, red meat, and processed foods.
Regular Exercise
150 min/week moderate exerciseAt least 150 minutes/week of moderate aerobic activity. Cardiac rehabilitation programs improve outcomes after ACS.
Weight Optimisation
BMI target <25 kg/m²Target BMI 18.5–25 kg/m². Weight loss improves BP, lipids, glycaemic control, and reduces angina symptoms.
Limit Alcohol
Maximum 14 units/weekAlcohol raises BP and provides no cardiovascular benefit. Limit to 1–2 units per day maximum.
Stress Management
Improves quality of lifeChronic stress and anxiety contribute to ischaemic heart disease. Relaxation techniques, yoga, and counselling help reduce symptom burden.
Guidelines & Latest Evidence
ESC and AHA guidelines inform the evaluation and management of chest pain.
Chest Pain Red Flags: When to Seek Emergency Care
Certain high-risk attributes indicate immediate life-threatening conditions like a heart attack.
Rest Chest Pain
Pain occurring without physical effort indicates unstable plaque — this is Acute Coronary Syndrome until proven otherwise.
New or Rapidly Worsening
Previously stable exertional discomfort that suddenly triggers with less effort or increases in duration and severity.
Associated Sweating or Nausea
Sweating (diaphoresis) during chest tightness is a strong objective indicator of significant myocardial ischaemia.
Syncope or Lightheadedness
Fainting or near-fainting during chest pain points to severe valve blockages (AS) or haemodynamic compromise.
Breathlessness in a Diabetic
Diabetic neuropathy can mask pain. Sudden exertional shortness of breath should be treated as equivalent to angina.
Neurological Deficits
Facial droop or arm weakness alongside chest tightness indicates poor perfusion or systemic aortic dissection.
Frequently Asked Questions
Guideline-directed clarifications regarding typical and atypical chest discomfort.
Cardiac chest pain is typically central or left-sided pressure, heaviness, or tightness — provoked by exertion or stress, lasting 2–15 minutes, with radiation to the left arm, jaw, or neck. Non-cardiac pain is more often sharp, very brief (<5 seconds), reproduced by pressing on the chest, or worse with breathing. However, symptoms overlap substantially — the only reliable way to distinguish cardiac from non-cardiac is formal assessment with ECG, blood tests, and echocardiography. Never self-diagnose chest pain as non-cardiac without a proper evaluation.
Go to emergency immediately if chest pain is: severe, new, or worst ever; accompanied by sweating, breathlessness, or nausea; radiates to the left arm, jaw, or back; persists more than 15 minutes at rest; is associated with fainting, light-headedness, or palpitations; or occurs with any neurological symptoms. Do not drive yourself — call 108. Chew aspirin (325 mg) if not allergic while awaiting help. For heart attacks, door-to-balloon time under 90 minutes dramatically improves outcomes — every minute of delay matters.
Initial evaluation includes: 12-lead ECG (first test — detects STEMI, prior MI, ischaemic changes); high-sensitivity troponin blood test (elevated in heart attack); chest X-ray. If acute coronary syndrome is excluded, further investigation includes 2D echocardiography (wall motion, valve disease), treadmill stress test or TMT (exercise-induced ischaemia), CT coronary angiography (non-invasive coronary anatomy), and invasive coronary angiography with FFR when pre-test probability is high or non-invasive tests are positive.
If you experience sudden or severe chest pain at rest, call emergency services (108 in India) immediately — do not drive yourself. While waiting, sit in a comfortable upright position, chew one adult aspirin (325 mg) if you are not allergic and have no contraindication, and loosen any tight clothing. Note the time the pain started and any associated symptoms such as sweating, breathlessness, or nausea. Do not eat or drink anything except a small sip of water with the aspirin. If you have been prescribed sublingual nitroglycerin, take one dose as directed. Rapid action saves heart muscle — every minute of delay increases permanent damage.
Stable angina is predictable chest tightness or pressure that occurs with exertion (e.g., walking uphill, climbing stairs) and reliably resolves within 5–15 minutes of rest or sublingual nitroglycerin. The coronary artery has a fixed narrowing that limits blood flow during increased demand but the plaque is stable. A heart attack (myocardial infarction) occurs when a plaque ruptures, forming a blood clot that suddenly blocks the artery completely — causing prolonged chest pain that does not resolve with rest, often accompanied by sweating, nausea, or breathlessness. Angina indicates risk; a heart attack indicates active muscle damage requiring emergency treatment.
Yes — anxiety and panic attacks can produce chest pain that closely mimics cardiac pain. Typical features include sharp or stabbing chest discomfort, a sense of impending doom, rapid breathing or hyperventilation, tingling in the hands or around the mouth, and palpitations. The pain may shift location and is often reproducible by pressing on the chest wall. However, because the symptoms can be indistinguishable from acute coronary syndrome, especially in patients over 40 or those with cardiac risk factors, it is essential to complete a proper cardiac evaluation — including ECG and troponin — before attributing chest pain to anxiety. Never self-diagnose chest pain as anxiety without a medical assessment.
Costochondritis is inflammation of the cartilage connecting the ribs to the breastbone (sternum). It produces sharp, localised chest pain that is typically reproducible by pressing firmly on the affected rib-joint area — a feature that is absent in cardiac pain. The pain may worsen with deep breathing, coughing, or certain arm movements. Costochondritis is benign and self-limiting, usually resolving within weeks with rest, anti-inflammatory medications, and ice or heat application. However, because the chest location overlaps with cardiac pain, anyone with new chest pain — especially those over 40 or with cardiac risk factors — should undergo ECG evaluation before assuming the cause is musculoskeletal.
Not every chest pain requires an ER visit, but certain features demand immediate emergency evaluation: pain that is severe, new, or the worst you have ever experienced; pain accompanied by sweating, breathlessness, nausea, or vomiting; pain that radiates to the left arm, jaw, neck, or back; pain that persists more than 15 minutes at rest; chest pain associated with fainting, light-headedness, or palpitations; or any chest pain in a patient with known heart disease, diabetes, or multiple cardiac risk factors. For mild, brief, reproducible chest pain in a young, healthy person with no risk factors, a scheduled outpatient evaluation is appropriate. When in doubt, err on the side of caution — call 108 or proceed to the ER.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.

Resting 12-Lead ECG
First-line test completed within minutes — detects ischaemia, arrhythmia, and prior MI.

2D Echocardiography
Wall motion assessment, valve disease, and pericardial evaluation.

Treadmill Stress Test
Exercise-induced ischaemia detection with Duke Treadmill Score.
Coronary Angiography
Definitive gold-standard imaging of coronary blockages with FFR.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.