
Heart Failure Management
Heart failure is a condition in which the heart cannot pump efficiently enough to meet the body's needs. Landmark guideline-directed medical therapy (GDMT) — the four pillars — can reduce mortality by over 50% when fully optimised.
What Is Heart Failure?
Heart failure is a clinical syndrome characterised by breathlessness, fluid retention, and chronic fatigue due to the heart's inability to pump efficiently.
It is not a standalone disease, but the endpoint of other chronic cardiovascular diseases. By measuring left ventricular ejection fraction (LVEF), we classify heart failure into HFrEF (reduced ejection fraction), HFmrEF (mildly reduced), and HFpEF (preserved pump function) to initiate specific, clinically proven pathways.
Common Causes & NYHA Functional Classes
Understanding what damaged your heart muscle is the first step in stopping the progression.
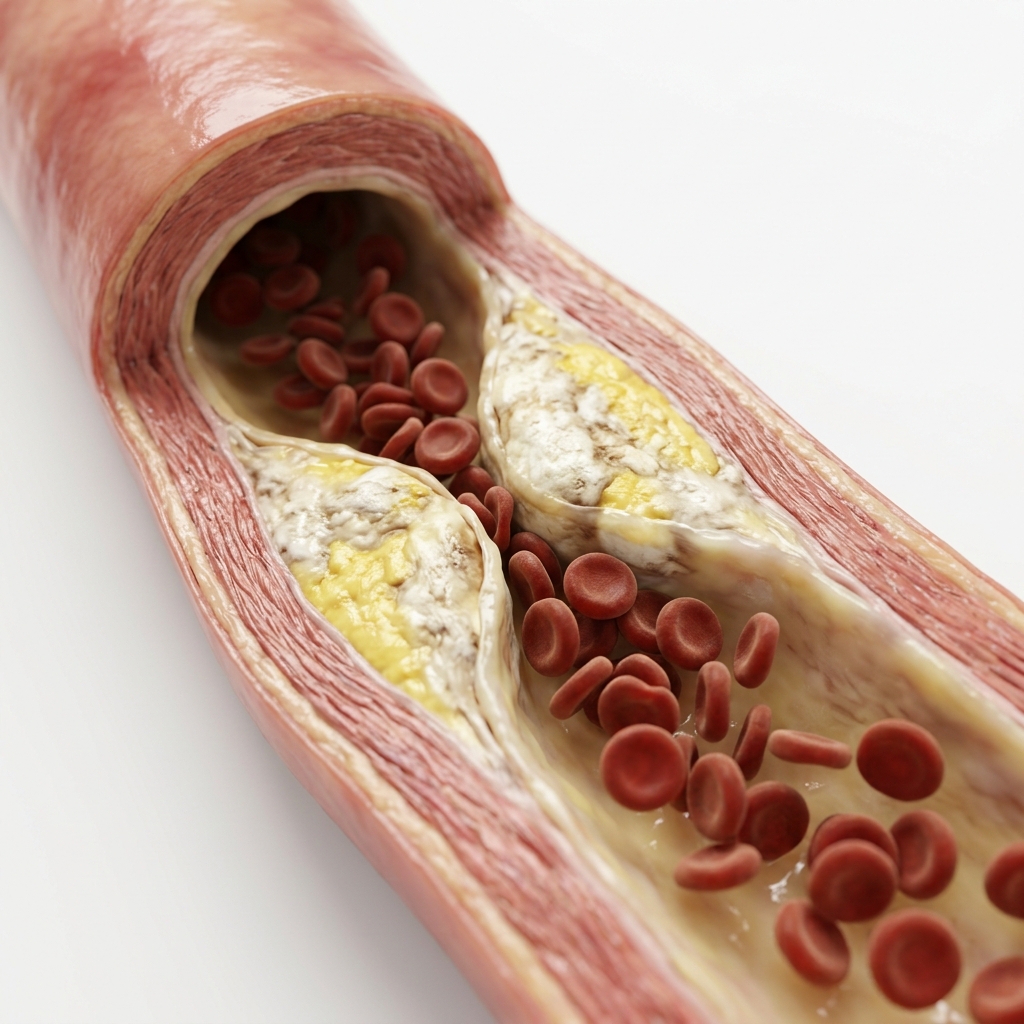
Coronary Artery Disease (CAD)
Prior heart attacks create permanent scar tissue, impairing contraction. Major driver of HFrEF (~70%).
Chronic Hypertension
Overworked ventricular muscle hypertrophies and stiffens, leading to HFpEF and eventual dilation.
Valvular Heart Disease
Mitral regurgitation or aortic stenosis causes progressive volume and pressure overload.
Cardiomyopathy
Dilated (DCM), hypertrophic (HCM), or restrictive patterns driven by genetics, virus, alcohol, or pregnancy.
Types & Severity of Heart Failure
Heart failure is classified by ejection fraction and functional capacity.
Classic Symptoms & Diagnostic Protocols
Classic signs include bilateral ankle swelling, breathlessness while lying flat (orthopnoea), and sudden nocturnal choking episodes.
Bilateral Ankle Swelling
Diagnostic MarkerRight-sided backlog causes dependent fluid build-up. One of the earliest and most recognisable signs of heart failure.
Orthopnoea / PND
Diagnostic MarkerSudden breathlessness when lying flat; relieved by sitting up. Paroxysmal nocturnal dyspnoea — waking suddenly gasping for air — is classic for HF.
Rapid Weight Gain
Warning SignSudden weight gain (>2kg in 3 days) points to fluid overload. Daily weight monitoring is a key self-care strategy.
Fatigue & Reduced Exercise Capacity
Common SymptomReduced cardiac output limits oxygen delivery to skeletal muscles, causing profound fatigue and exercise intolerance.
How Is Heart Failure Diagnosed?
A combination of clinical assessment, biomarkers, and imaging confirms the diagnosis.
2D Echocardiography
Measures EF, diastolic function (E/e'), valve disease, and pulmonary pressure. The single most important diagnostic test for heart failure.
NT-proBNP / BNP Blood Test
Blood marker. Elevated values (>125 pg/mL NT-proBNP) confirm clinical heart failure. Rules out HF when normal, with high negative predictive value.
12-Lead ECG
Identifies LBBB (CRT eligibility), prior infarcts (Q waves), LVH, and arrhythmias. A normal ECG makes HFrEF unlikely.
Chest X-Ray
Detects cardiomegaly (enlarged heart) and pulmonary congestion (fluid in lungs). Quick and widely available.
Coronary Angiography
Rules out or confirms CAD (ischaemic cardiomyopathy) as the root cause of LV dysfunction.
What Happens If Left Untreated?
Progressive heart failure leads to worsening symptoms, frequent hospitalisation, and reduced survival.
Progressive LV Dysfunction
Without GDMT, the left ventricle continues to dilate and remodel. EF declines further, and symptoms progress from NYHA I to IV.
Refractory Fluid Overload
Persistent pulmonary and systemic congestion leads to repeated hospitalisations for intravenous diuretics. Quality of life deteriorates.
Cardiorenal Syndrome
Reduced cardiac output worsens renal perfusion, causing diuretic resistance and progressive renal failure.
Sudden Cardiac Death
Advanced heart failure carries high risk of ventricular arrhythmias. ICD implantation is life-saving in appropriate patients.
The 4 Pillars of GDMT Therapy
Guideline-Directed Medical Therapy (GDMT) uses four drug classes in synergistic combination to halt remodelling and extend survival.
ARNi / ACEi / ARB
PARADIGM-HF: −20% CV DeathSacubitril-Valsartan (Entresto) blocks the renin-angiotensin-aldosterone system. Superior to ACE inhibitors, reducing CV death and hospitalisation by 20%.
Beta-Blockers
MERIT-HF: −34% MortalityBisoprolol, Carvedilol, Metoprolol Succinate. Blunts sympathetic overdrive and slows heart rate, allowing the ventricle to recover. MERIT-HF: −34% all-cause mortality.
MRA Therapy
EMPHASIS-HF: −37% CV EventsSpironolactone / Eplerenone. Prevents aldosterone-driven fibrotic scarring and sodium retention. EMPHASIS-HF: −37% CV events.
SGLT2 Inhibitors
DAPA-HF: −26% Worsening HFDapagliflozin / Empagliflozin. Reduce worsening HF or CV death by 26% (DAPA-HF) in all HF patients, regardless of diabetes status.
Heart Failure Medication Pillars
Four drug classes work together to reduce mortality and hospitalisation.
Lifestyle Changes & Self-Care for Heart Failure
Daily self-monitoring and healthy habits are essential for maintaining stability.
Daily Weight Monitoring
Early warning for decompensationWeigh yourself every morning before breakfast. A gain of >2 kg in 3 days indicates fluid overload requiring medication adjustment.
Salt Restriction
Reduces fluid overloadLimit sodium to <2g per day. Avoid processed foods, canned goods, and restaurant meals. Salt causes fluid retention and worsens congestion.
Structured Exercise Program
Improves functional capacityCardiac rehabilitation improves functional capacity and quality of life. Start with walking and gradually increase as tolerated.
Limit Alcohol & Fluids
Individualised restrictionAlcohol depresses cardiac function. Fluid restriction (1.5–2 L/day) may be needed in advanced HF with hyponatraemia.
Sleep & Breathing Management
CPAP improves outcomesSleep on an incline (2–3 pillows) to reduce orthopnoea. Screen for sleep apnoea which worsens HF outcomes.
Vaccination & Infection Prevention
Annual flu + pneumococcal vaccineInfluenza and pneumococcal vaccines are recommended. Respiratory infections are a common trigger for HF decompensation.
Guidelines & Latest Evidence
Landmark trials have transformed heart failure from a terminal diagnosis to a manageable chronic condition.
When to See a Doctor
Certain symptoms indicate worsening heart failure requiring prompt medical attention.
Sudden Weight Gain (>2 kg in 3 Days)
Rapid fluid accumulation indicates worsening congestion. Diuretic adjustment may be needed to prevent hospitalisation.
Worsening Breathlessness or Orthopnoea
Increasing difficulty breathing, needing more pillows to sleep, or waking up gasping for air suggests decompensation.
Chest Pain or Palpitations
New chest pain or palpitations in a heart failure patient require ECG evaluation to rule out ACS or arrhythmia.
Reduced Exercise Tolerance
If you cannot walk as far or climb as many stairs as before, this may signal worsening HF requiring treatment adjustment.
Frequently Asked Questions
Guideline-directed answers regarding chronic heart failure and devices.
Heart failure is a clinical syndrome in which the heart cannot pump efficiently enough to meet the body's demands — or can only do so at abnormally elevated filling pressures. The result is breathlessness, ankle swelling, and fatigue. It is not a disease in itself but a consequence of underlying conditions — most commonly coronary artery disease, hypertension, or valve disease. Modern guideline-directed therapy has transformed heart failure into a manageable chronic condition where mortality can be reduced by over 50% with optimal treatment.
Ejection fraction (EF) is the percentage of blood pumped out of the left ventricle with each heartbeat, measured by echocardiography. Normal EF is 55–70%. Heart failure is classified by EF: HFrEF (EF <40%), HFmrEF (EF 40–49%), and HFpEF (EF ≥50%). The classification determines treatment — HFrEF responds strongly to all four GDMT pillars with proven mortality benefits. HFpEF is managed differently, primarily with SGLT2 inhibitors and risk factor control.
The four pillars of GDMT for HFrEF are: (1) ACEi/ARNi — sacubitril-valsartan; (2) Beta-blockers — bisoprolol, carvedilol, or metoprolol succinate; (3) MRA — spironolactone or eplerenone; (4) SGLT2 inhibitors — dapagliflozin or empagliflozin. All four classes together produce additive benefits, reducing cardiovascular mortality by over 55% compared with placebo.
SGLT2 inhibitors (dapagliflozin, empagliflozin) were originally diabetes medications but were found in large trials to dramatically reduce heart failure outcomes independent of glucose lowering. DAPA-HF (NEJM 2019) showed dapagliflozin reduced worsening HF or CV death by 26% in HFrEF patients — including those without diabetes. They are now recommended for all HFrEF patients, regardless of diabetes status.
Yes — heart failure can improve significantly with optimal guideline-directed medical therapy (GDMT). The four pillars of treatment — ARNi/ACEi, beta-blockers, MRAs, and SGLT2 inhibitors — work together to reduce the workload on the heart, block harmful neurohormonal activation, and promote reverse cardiac remodelling. Many patients experience improvement in ejection fraction (sometimes normalising from severely reduced levels), reduction in heart size, and resolution of symptoms. This is called 'heart failure with recovered EF'. However, heart failure remains a chronic condition — even when EF normalises, medication is typically continued lifelong to maintain the improvement and prevent recurrence.
Fluid management in heart failure depends on the severity of the condition. For patients with stable, well-compensated heart failure, a standard fluid intake of 1.5–2 litres per day is generally acceptable. For patients with moderate-to-severe heart failure, especially those requiring high-dose diuretics or with recurrent fluid overload, fluid restriction to 1.5 litres per day is often recommended. More importantly than fluid intake, salt restriction below 5 g per day is critical — salt drives fluid retention. Daily weight measurement is the most practical way to monitor fluid status: a weight gain of more than 2 kg in 3 days indicates fluid overload requiring medical attention.
Yes — regular exercise is not only safe for most patients with stable heart failure, it is strongly recommended. Exercise training improves exercise capacity, quality of life, and reduces hospitalisation rates. The ESC recommends at least 30 minutes of moderate-intensity aerobic exercise (such as brisk walking or stationary cycling) on most days, supplemented by resistance training twice weekly. Cardiac rehabilitation programmes provide supervised, individualised exercise prescription. Patients should avoid heavy lifting, straining, and high-intensity isometric exercises — particularly those with reduced EF or device implants. Always obtain clearance from your cardiologist before starting an exercise programme, especially if you have advanced heart failure.
End-stage (Stage D) heart failure is advanced heart failure with persistent severe symptoms despite maximal medical therapy and device optimisation. Options include advanced therapies and palliative care. Left ventricular assist devices (LVADs) are mechanical pumps that support the failing heart — used as a bridge to transplant or as destination therapy. Heart transplantation remains the definitive treatment for eligible candidates. For patients who are not candidates for advanced therapies, palliative care focused on symptom management, quality of life, and advance care planning is an essential component. Continuous inotropic support at home may be considered in select cases. Early referral to a heart failure specialist centre is critical for patients with advanced disease.
“Advanced cardiovascular care. Restoring life, rhythm, and vitality.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management for this condition at Heartwise Cardiology Clinic, Vashi.

2D Echocardiography
EF measurement, diastolic function, valve disease, and pulmonary pressures.

CRT & ICD Therapy
Biventricular pacing and defibrillator implantation for advanced HF.

MitraClip Repair
Transcatheter mitral valve repair for secondary MR in heart failure.
Coronary Artery Disease
Ischaemic cardiomyopathy evaluation and revascularisation options.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.