Coronary Angioplasty & Stenting
IVUS & OCT-Guided · Radial-First Protocol · Kokilaben Hospital, Koperkhairne. Coronary angioplasty and stenting — also called Percutaneous Coronary Intervention (PCI) — is a minimally invasive procedure that opens blocked or narrowed coronary arteries by inflating a small balloon catheter and deploying a drug-eluting stent to hold the artery permanently open.
What is Angioplasty & Stenting?
An evidence-based overview of Percutaneous Coronary Intervention (PCI) and the mechanics of drug-eluting stents.
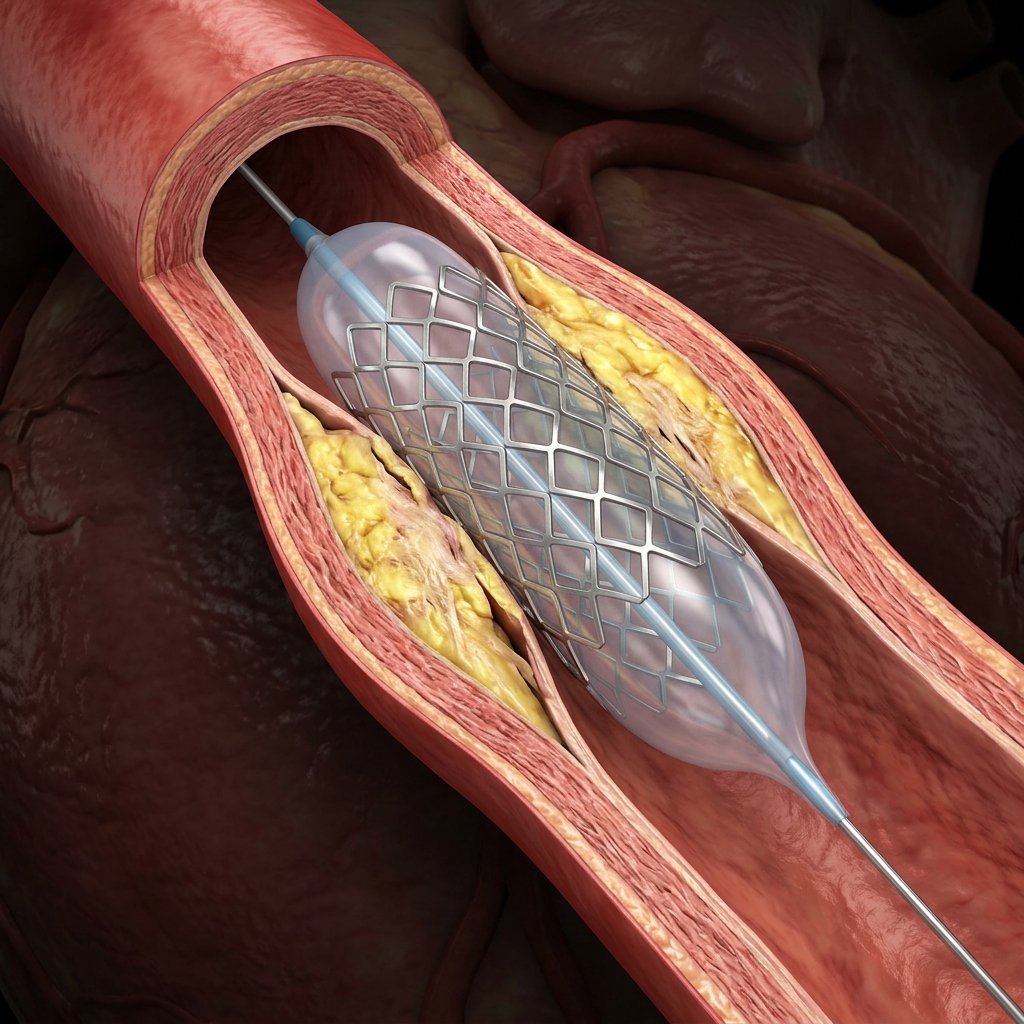
Coronary angioplasty and stenting — formally called Percutaneous Coronary Intervention (PCI) — is a catheter-based procedure that restores blood flow through a narrowed or blocked coronary artery without open-heart surgery. A deflated balloon catheter is advanced to the blockage, inflated to compress the plaque, and then a drug-eluting stent (a tiny metallic mesh tube coated with medication) is deployed to hold the artery permanently open. Modern drug-eluting stents release anti-proliferative drugs (everolimus, zotarolimus, or sirolimus) over 3–6 months to prevent scar tissue forming inside the stent — reducing the restenosis rate from 20–40% (bare metal stents) to less than 5% at one year. The procedure is performed in a Cardiac Catheterisation Laboratory (Cath Lab) under local anaesthesia and mild sedation. The catheter is typically introduced through the radial artery at the wrist — the transradial approach — which allows patients to sit up and move immediately after the procedure, with most discharged the same day. When angioplasty is NOT the right answer: For complex three-vessel disease with high SYNTAX score, or left main disease with certain anatomy, coronary bypass surgery (CABG) may produce better long-term outcomes. Dr. Amit Singh makes this recommendation transparently when the evidence supports it — even if it means referring the patient for surgery rather than performing angioplasty.
Clinical Indications & Urgency Profiles
Understanding when coronary angioplasty is indicated based on symptom acuity and lesion characteristics.
IVUS & OCT Guidance: Evidence-Based Medicine
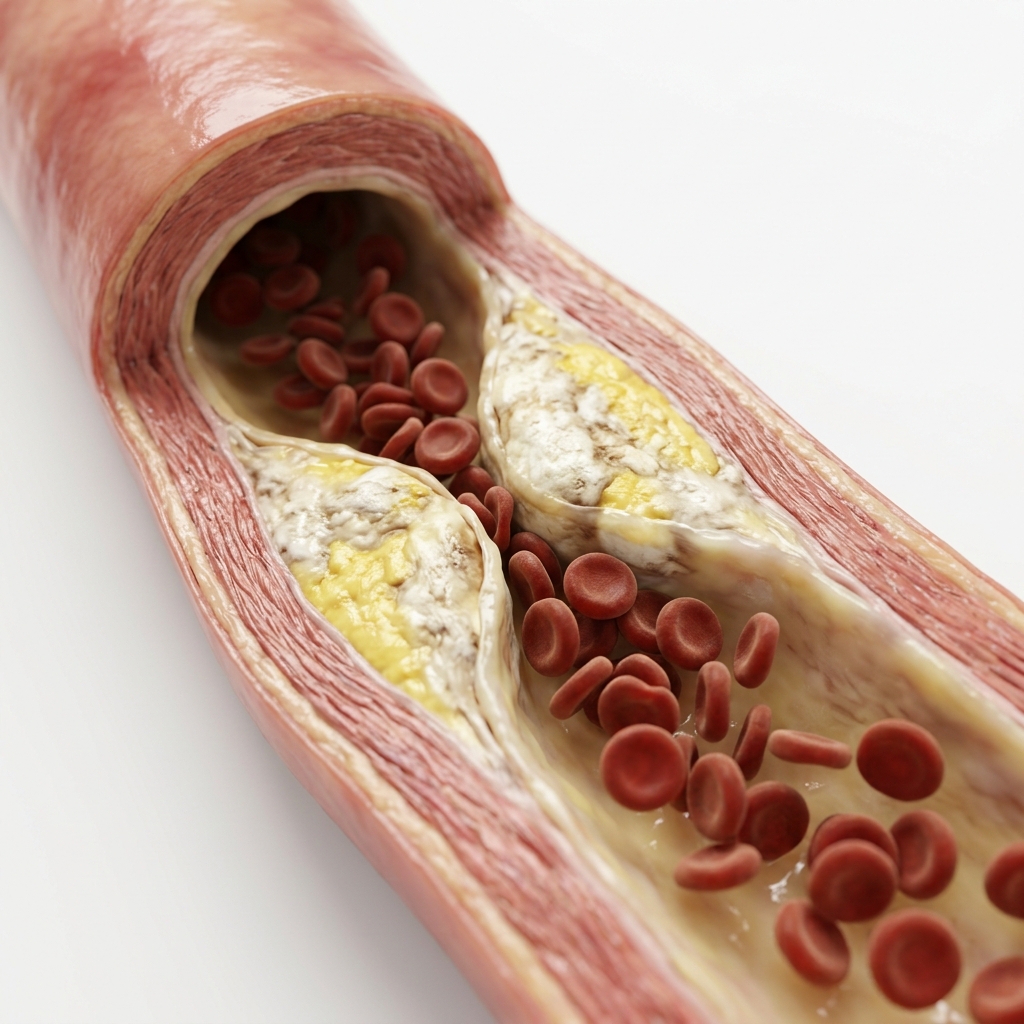
Standard angiography only provides a 2D shadow of the vessel. Intravascular ultrasound (IVUS) and Optical Coherence Tomography (OCT) inspect the arterial walls from the inside, confirming flawless stent positioning and sizing.
IVUS-guided drug-eluting stent placement vs standard angiography-guided PCI for complex coronary lesions.
Reduction in major adverse cardiac events (MACE) at 3 years with IVUS guidanceOCT-guided PCI versus angiography-guided PCI for complex lesions in an all-comers randomised trial.
2-year MACE with OCT guidance vs 2.69% with angiography guidanceOCT-guided PCI versus angiography-guided PCI specifically for bifurcation coronary lesions.
Relative reduction in 2-year MACE with OCT-guided bifurcation PCIComplex PCI: Rotablation, IVL & CTO
The full therapeutic spectrum of advanced coronary interventions, designed for highly calcified blockages, branching vessels, and chronic total occlusions.
Calcified Coronary Lesions
01Severely calcified arteries cannot be adequately dilated with a standard balloon — the calcium prevents stent expansion. Intravascular Lithotripsy (IVL) uses pulsatile sonic pressure waves to fracture calcium from inside the vessel, enabling stent deployment. Rotational atherectomy (Rotablation) uses a diamond-tipped burr to ablate calcified plaque.
Bifurcation PCI
02Bifurcation lesions involve a blockage at the junction where a main coronary artery divides into a branch. Treating bifurcations requires specific stenting strategies — provisional T-stenting, DK-Crush, or Culotte techniques — to maintain flow in both the main vessel and the branch. OCT guidance is particularly valuable to confirm final result.
Left Main Coronary PCI
03The left main coronary artery supplies 70–80% of the heart muscle's blood supply. Left main disease historically required bypass surgery (CABG). The EXCEL trial established that in selected patients with low-to-intermediate SYNTAX scores, left main PCI achieves comparable outcomes to CABG at 5 years.
Chronic Total Occlusion (CTO)
04A Chronic Total Occlusion is a coronary artery that has been completely blocked for over 3 months. CTOs are the most technically challenging lesions in interventional cardiology. CTO PCI uses antegrade and retrograde wire crossing strategies to re-canalise the vessel.
Multi-Vessel PCI
05In patients with multiple significant blockages — two or three vessels simultaneously — a decision must be made about whether to treat all vessels or only the culprit lesion. FFR (Fractional Flow Reserve) guidance is essential: the FAME 2 trial established that treating only FFR-positive lesions produces better outcomes.
In-Stent Restenosis (ISR)
06In-stent restenosis occurs when scar tissue grows inside a previously placed stent, re-narrowing the vessel. OCT is the imaging tool of choice for ISR evaluation — identifying whether the mechanism is under-expansion, neointimal hyperplasia, or neoatherosclerosis — which determines the correct therapeutic strategy.
Drug-Eluting Stents: Which & Why
Detailed comparison of second-generation drug-eluting stents (DES) used across clinical scenarios.
Everolimus-Eluting Stent
Everolimus (mTOR inhibitor)
Technical Specs
- •Restenosis rate: <5% at 1 yr
- •DAPT duration: 6–12 months
- •Stent thrombosis: <0.5% / year
Zotarolimus-Eluting Stent
Zotarolimus (mTOR inhibitor)
Technical Specs
- •Restenosis rate: <5% at 1 yr
- •DAPT — high bleed risk: 1 month possible
- •Stent thrombosis: <0.6% / year
Sirolimus-Eluting Stent
Sirolimus (mTOR inhibitor)
Technical Specs
- •Restenosis rate: <5% at 1 yr
- •Strut thickness: 60–80 µm
- •Stent thrombosis: <0.5% / year
How to Prepare for Angioplasty
Critical guidelines to follow during the days leading up to your cardiac catheterisation procedure.
What Happens During Angioplasty?
Detailed workflow of your intervention — from local anesthesia to final imaging confirmation.
Preparation & Radial Access
Local anaesthetic at the wrist. Radial artery puncture with a small needle. A 6Fr or 7Fr sheath is placed to provide access. IV heparin (anticoagulation) is administered. Continuous ECG and BP monitoring throughout.
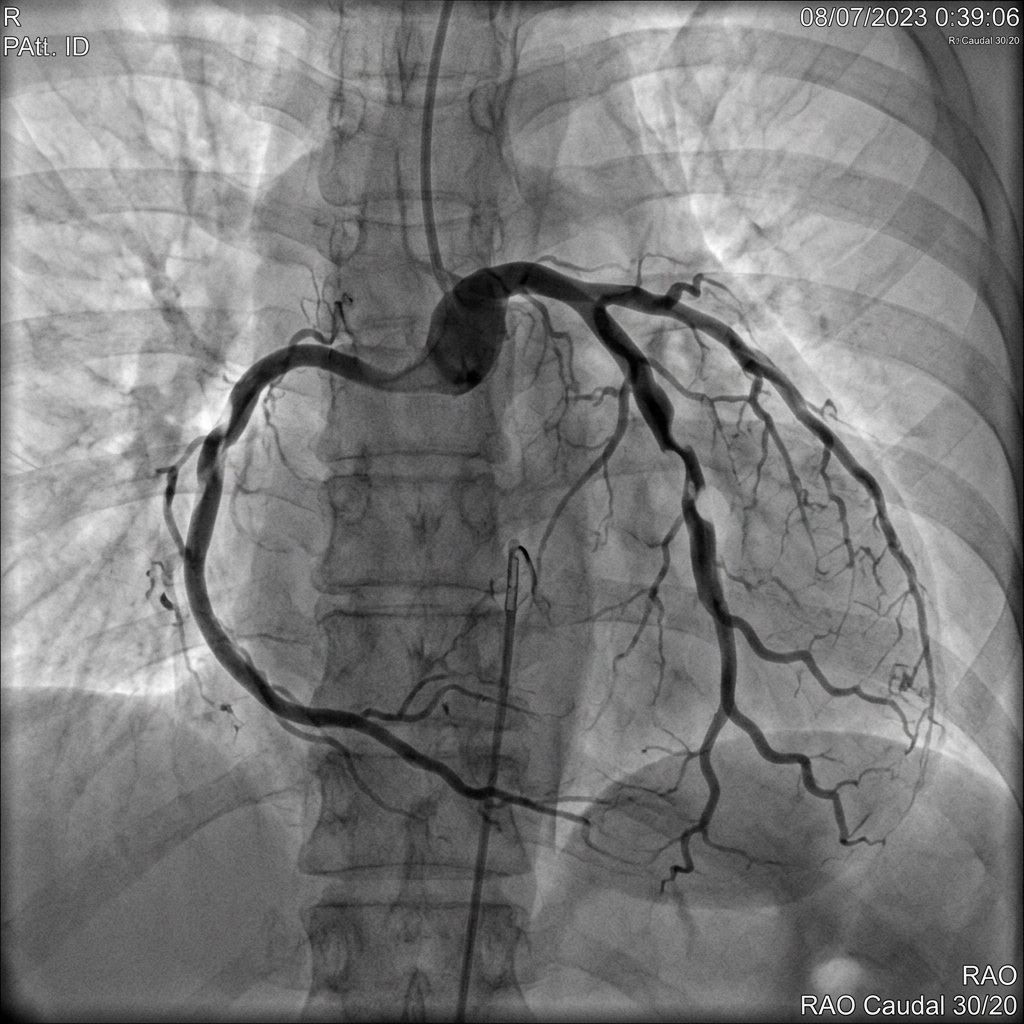
Diagnostic Angiography
If not already done, coronary angiography is performed first to confirm the target lesion, assess other vessels, and plan the intervention. SYNTAX score is calculated for complex multi-vessel cases.
Guidewire Crossing
A coronary guidewire (0.014") is advanced through the guide catheter and across the blockage into the distal vessel. This is the most critical technical step — the wire must cross safely without perforating the vessel.
Pre-dilation (Balloon Angioplasty)
A semi-compliant balloon catheter is advanced to the lesion and inflated at 8–14 atmospheres to open the blockage. In calcified lesions, IVL or rotational atherectomy is performed at this stage before stenting.
IVUS / OCT Imaging (Pre-stent)
An IVUS or OCT catheter is advanced to the lesion to measure the true vessel diameter, assess plaque characteristics, and determine optimal stent length and diameter. This step eliminates guesswork from stent sizing.
Stent Deployment
The appropriately sized drug-eluting stent is advanced to the lesion and deployed at high pressure (typically 12–16 atmospheres). The stent expands and is left permanently in the artery.
Post-dilation & IVUS/OCT Confirmation
A non-compliant balloon post-dilates the stent to ensure complete expansion. Final IVUS or OCT imaging confirms optimal stent apposition, full expansion, and absence of edge dissection or under-expansion.
Sheath Removal & Recovery
The sheath is removed. A wrist compression band is applied for 2–3 hours. The patient is monitored in the recovery area. Results and next steps are discussed with the patient and family within 1–2 hours.
Benefits & Risks of Coronary Angioplasty
A scientific, transparent perspective on procedural outcomes and safety profiles.
Core Clinical Benefits
- Immediate relief of angina (chest pain) in >90% of patients with significant stenosis
- Reduces risk of future heart attack in haemodynamically significant lesions (FAME 2 trial)
- No open-chest surgery — no sternotomy, no general anaesthesia, minimal discomfort
- Radial approach: fully ambulatory within 1–2 hours, same-day discharge possible
- Procedure completed in 45–90 minutes in most cases
- Drug-eluting stents: <5% restenosis rate — durable, highly reliable long-term result
- Life-saving in heart attack (STEMI) — every 30 minutes saved reduces patient mortality
- IVUS/OCT guidance: reduces need for repeat procedures by 25% or more
Potential Risks & Incidence
- Contrast nephropathy: <1% with adequate hydration and modern low-osmolar contrast
- Access-site bleeding: <1–2% with radial approach (vs 3–5% femoral)
- Coronary artery dissection: rare (<0.1%); usually managed with immediate additional stenting
- Acute stent thrombosis: <0.5% / year; risk highest if DAPT stopped early
- Stroke: <0.1% for elective PCI at experienced centres
- Emergency CABG: <0.1% (very rare with modern interventional techniques)
- Death: <0.1% for elective PCI; higher in emergency heart attack setting
- Stent restenosis: <5% at 1 year with DES; managed with DCB or repeat stenting
Recovery & DAPT Guidelines
Standard timeline for recovery and the critical importance of Dual Antiplatelet Therapy (DAPT) in preventing stent thrombosis.
IVUS vs OCT vs Angiography
Comparison of intravascular imaging modalities for optimal stent deployment guidance.
Post-PCI Outcome Assessment
Interpretation of procedural results after coronary angioplasty and stenting.
Frequently Asked Questions
Detailed, peer-reviewed answers to the most common patient concerns regarding stenting and long-term care.
For most single-vessel or two-vessel coronary artery disease, angioplasty with drug-eluting stenting is preferred over bypass surgery — it is less invasive, has a shorter recovery, and achieves equivalent outcomes for most patients. For complex three-vessel disease or left main disease, the SYNTAX and EXCEL trials show bypass surgery may offer better long-term results in selected patients with high SYNTAX scores. The decision is individualised — Dr. Amit Singh will recommend the option the evidence supports for your specific anatomy.
IVUS (Intravascular Ultrasound) places a miniature ultrasound probe inside the coronary artery to visualise the vessel wall in cross-section during the procedure. This allows the cardiologist to correctly size the stent, confirm complete expansion, and detect complications invisible on plain angiography. The RENOVATE trial (NEJM 2023, 1,639 patients) demonstrated IVUS-guided PCI reduces major adverse cardiac events by 25% versus angiography-guided PCI alone. Dr. Amit Singh uses IVUS or OCT guidance routinely at Kokilaben Hospital, Koperkhairne.
A coronary stent is a permanent metallic implant — it stays in the artery for life and does not need replacement. Modern drug-eluting stents have a restenosis (re-narrowing) rate of less than 5% at one year, compared to 20–40% for older bare-metal stents. With proper dual antiplatelet therapy and cardiovascular risk factor control (statins, blood pressure management, diabetes control, smoking cessation), most patients do not require repeat intervention in the stented segment.
DAPT means taking two antiplatelet medications simultaneously — aspirin plus clopidogrel, ticagrelor, or prasugrel. After drug-eluting stent placement, ACC/AHA guidelines recommend 6–12 months of DAPT for stable coronary artery disease and 12 months after a heart attack. DAPT prevents blood clots from forming on the stent while it heals. Never stop DAPT early without consulting your cardiologist — premature cessation is the leading cause of acute stent thrombosis, a serious complication.
After radial-approach coronary angioplasty, most patients are mobile within 1–2 hours and discharged the same day or after an overnight stay. Avoid heavy lifting and strenuous exercise for 1–2 weeks. Return to desk work is typically possible within 3–5 days. Driving is permitted after 24–48 hours. Full physical activity is resumed within 2–4 weeks. Follow-up is at 1 month, 3 months, and annually.
Yes — coronary angioplasty is safe and effective in diabetic patients. Diabetic patients often have more calcified and diffuse coronary disease, requiring advanced techniques such as IVUS/OCT guidance, intravascular lithotripsy (IVL), or rotational atherectomy. Modern everolimus-eluting stents perform well in diabetic vasculature. Metformin should be stopped 24–48 hours before and restarted 48 hours after the procedure, once kidney function is confirmed stable.
Yes. Coronary angioplasty and stenting is a listed procedure covered by most Indian health insurance policies, including cashless treatment. CGHS, ECHS, and Ayushman Bharat PM-JAY cover the procedure for eligible patients at Kokilaben Dhirubhai Ambani Hospital, Koperkhairne. Most private health insurers (Star Health, New India, ICICI Lombard, HDFC Ergo) also provide coverage. Pre-authorisation from your insurer is typically required before the procedure. Contact Heartwise Cardiology on 9769517636 for insurance guidance.
Coronary angioplasty is a safe, routinely performed procedure with a major complication rate of less than 1% at experienced centres. Stroke risk is less than 0.1%. Emergency surgery is required in less than 0.1% of cases. The procedure is performed in a dedicated Cardiac Catheterisation Laboratory at Kokilaben Hospital, Koperkhairne, with continuous monitoring, full resuscitation equipment, and an experienced interventional cardiology team. The radial (wrist) access approach reduces access-site bleeding by 73% compared to femoral access (RIVAL trial).
“Precision in structural interventions. Excellence in clinical outcomes.”

Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Cardiac Services Available at Heartwise
Dr. Amit Singh offers comprehensive cardiac diagnostics and management at Heartwise Cardiology Clinic, Vashi.
Coronary Angiography
Diagnostic coronary angiography with FFR and IVUS guidance.

Treadmill Stress Test
Exercise ECG to assess ischaemia before and after angioplasty.

2D Echocardiography
Post-angioplasty LV function assessment and wall motion evaluation.
Coronary Artery Disease
CAD diagnosis, medical management, and revascularisation planning.
Book a Visit.
Pick a date and time that works for you.
Select a date
| Su | Mo | Tu | We | Th | Fr | Sa |
|---|---|---|---|---|---|---|
Book an Appointment with Dr. Amit Singh, FACC.
Schedule a cardiology consultation at Heartwise Clinic in Vashi, Navi Mumbai — online booking, WhatsApp, or call. Dr. Amit Singh offers in-clinic and secure video teleconsultations for patients across India and internationally.
Choose Date & Time
Pick a slot that fits your schedule from available morning or evening appointments.
Share Your Details
Provide your name, contact number, and a brief note about your cardiac concern or reason for visit.
Get Confirmed
Our clinical team confirms your slot within 24 hours via call or WhatsApp with pre-visit instructions.
Consult In-Clinic or Online
Visit Heartwise Clinic in Vashi or join a secure HD video teleconsultation from anywhere.
Consultation Options
In-Clinic Consultation
Kokilaben Hospital, Kopar Khairane & Heartwise Clinic, Vashi
HD Video Teleconsultation
Available pan-India and for international patients
WhatsApp Booking
Quick booking via +91 97695 17636 — reports & follow-ups
100+ appointments this month
Confirmed by our clinical team
4.9 / 5 rating
From patient reviews
Our Cardiology
Centers.
Dr. Amit Singh consults across multiple flagship centers and outreach clinics in Navi Mumbai & Dombivli to ensure specialized, top-tier cardiac care is directly accessible.
Navi Mumbai Sectors & Surrounding Nodes Served
Triple ESC & FACC Certified
International guidelines and clinical safety protocols applied across all heart centers.
“Beat Better. Live Wiser.”
Dr. Amit Singh, FACC
Consultant Interventional Cardiologist
Medical Disclaimer: This article has been written and reviewed by Dr. Amit Singh, FACC, for educational purposes only. It does not constitute personalised medical advice and should not be used as a substitute for a consultation with a qualified cardiologist. Individual clinical decisions must be made by a treating physician based on complete medical history and examination. If you are experiencing chest pain, breathlessness, or other cardiac symptoms, seek emergency medical care immediately.